l l l respiratory muscle dysfunction recurrent aspiration
 thromboembolic events Inflammation")

 SSc PM/DM RA SLE SS MCTD 寻常型间质性肺炎(UIP) RA SSc PM/DM SS")






















. 155 (80 NAC")
 and 51/75 taking placebo (68%) completed one year")
. There")

- Slides: 59
影响肺功能 l l l respiratory muscle dysfunction recurrent aspiration (esophageal dysmotility) thromboembolic events Inflammation of the cricoarytenoid joints or development of bronchiectasis.
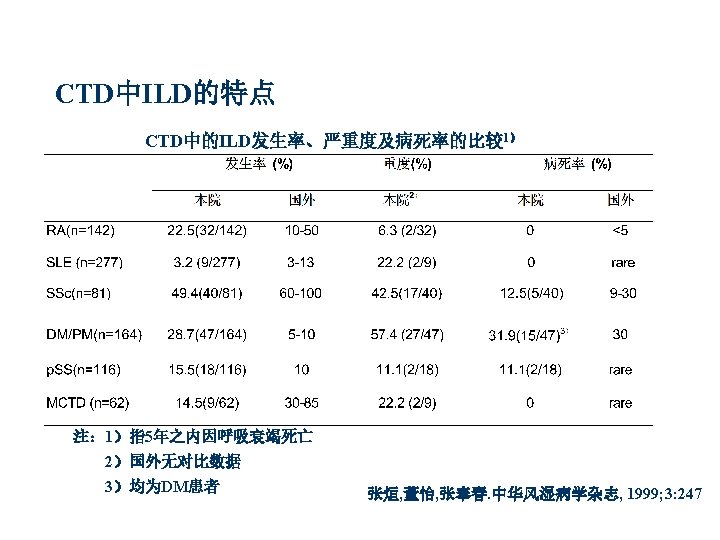
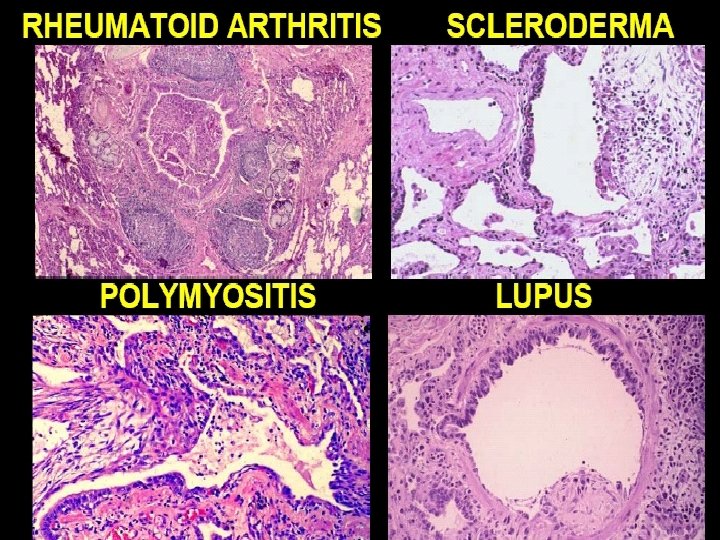
ILD的发生率 l l l 15%的CTD合并ILD 70% SSc合并肺部病变,2年内可发展为ILD, 组织病理77. 5%SSc伴ILD 10%DM/PM合并ILD 胸片显示 3. 7%RA合并ILD SLE,SS,MCTD Clin Chest Med 2004; 25: 549 ~ 559 Am J Respir Crit Care Med 2002; 165: 1581 ~ 6 Ann Rheum Dis 2003 ; 62 : 897 ~ 900
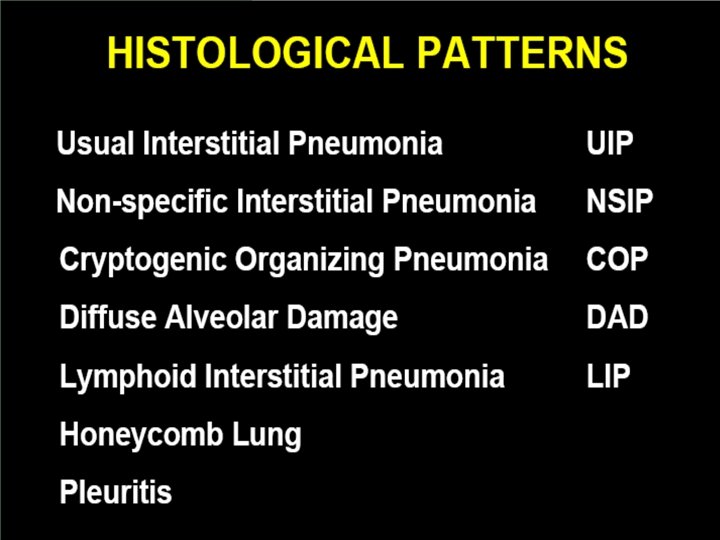
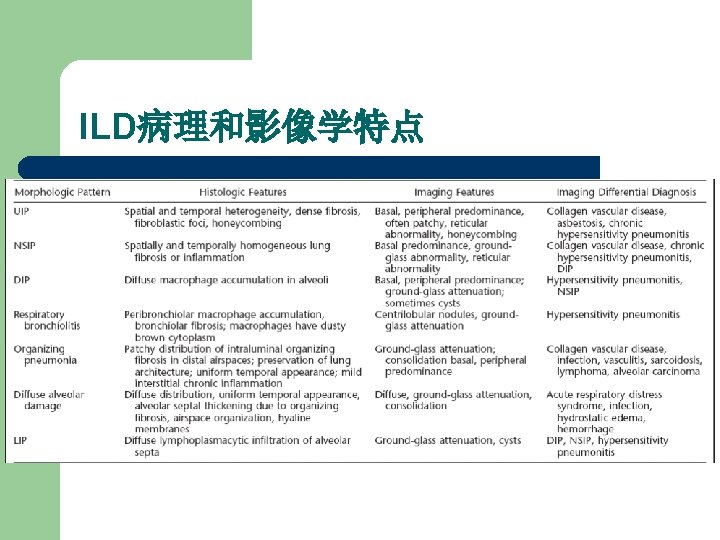
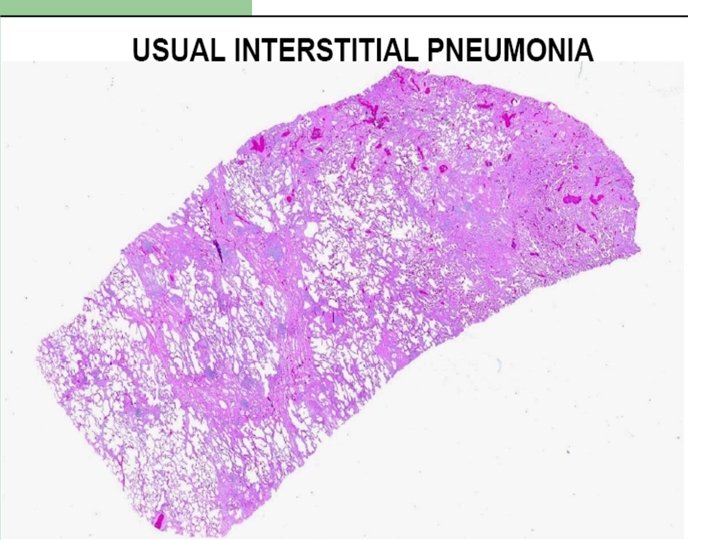
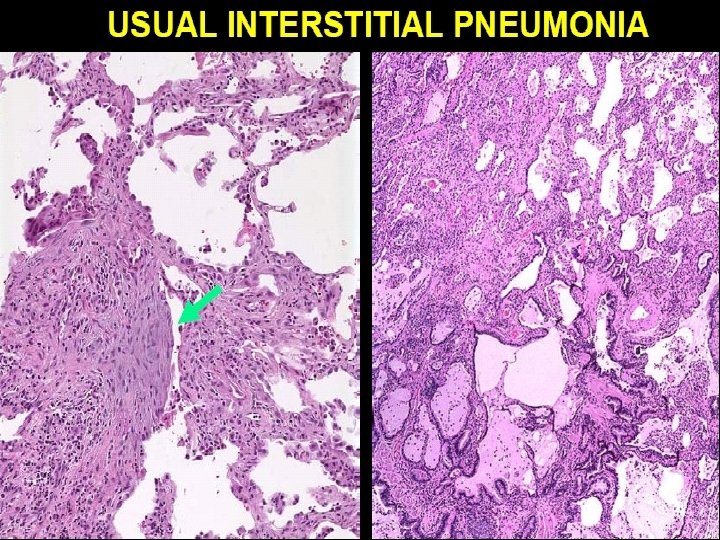
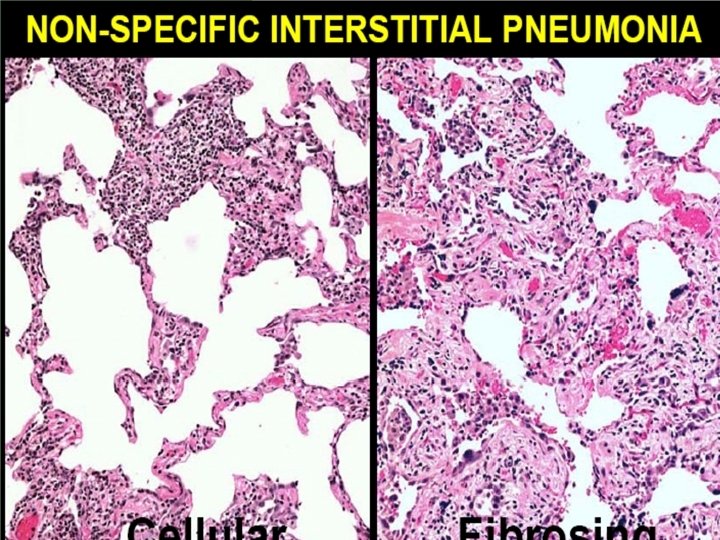
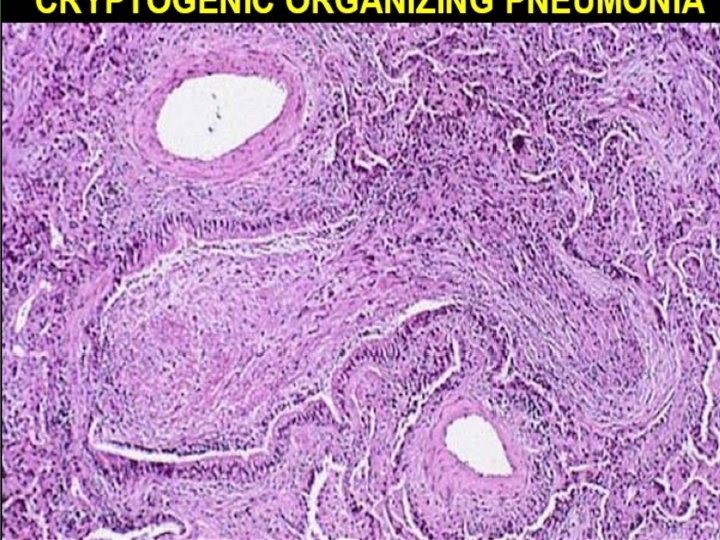
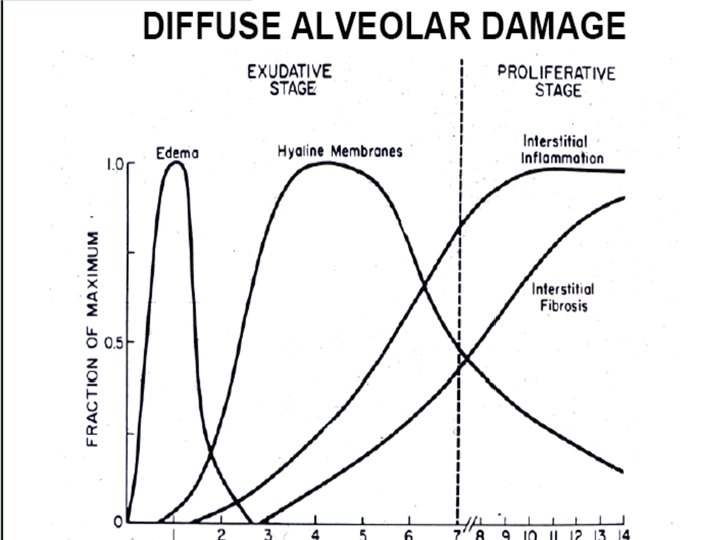
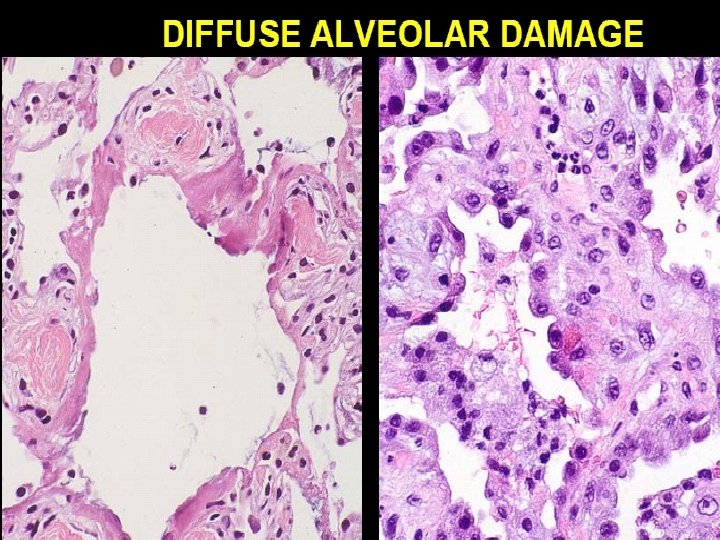
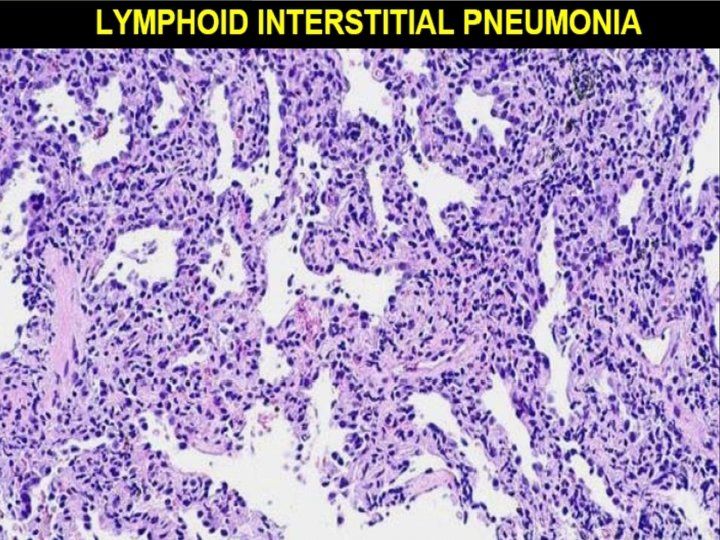
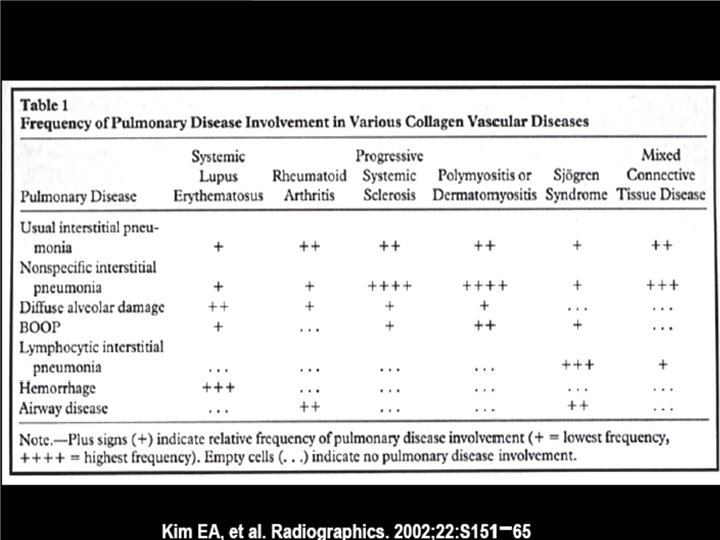
ILD的分类 易发生的疾病 非特异性间质性肺炎(NIP) SSc PM/DM RA SLE SS MCTD 寻常型间质性肺炎(UIP) RA SSc PM/DM SS 机化型肺炎(OP) PM/DM RA SSc SLE SS 淋巴细胞浸润性肺炎(LIP) SS SLE RA MCTD 脱屑性间质性肺炎(DIP) SLE RA SSc 弥漫性肺泡炎(DAD) SLE SSc PM/DM RA MCTD Curr Opin Rheumtol 2004; 16: 186 ~ 191
HRCT - non-specific interstitial pneumonia Systemic sclerosis DM/PM
HRCT - usual interstitial pneumonia Systemic sclerosis RA DM/PM
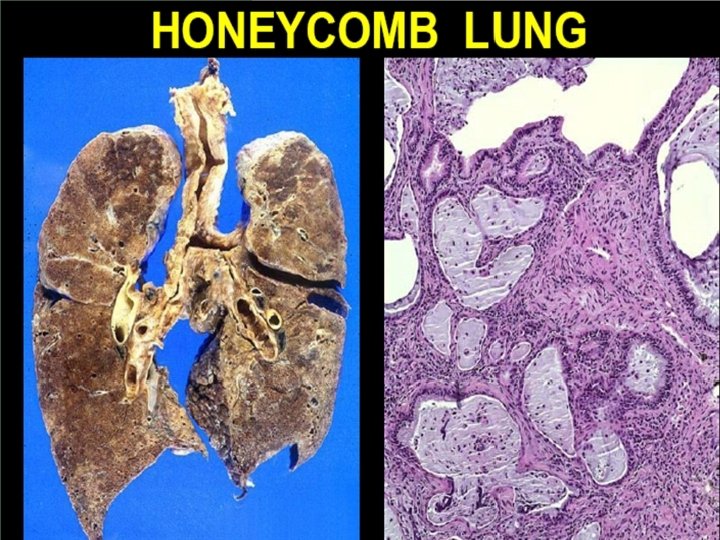
UIP-HRCT特点 l l patchy pattern of peripheral “honeycombing” more prominent in the bases of the lungs, traction bronchiectasis absence of prominent ground-glass opacity.
HRCT - chronic lymphocytic interstitial pneumonia Sjogren’s syndrome RA Drug induced
HRCT obliterative bronchiolitis RA SLE Scleroderma PM/DM
HRCT organizing pneumonia Gold SSZ MTX Sjogren’s syndrom RA
HRCT a patient with RA 33% of with RA associated parenchymal lung disease 31 IPF Radiography: 2 -6% 29 HRCT: 10% - 47% 35 -8 HRCT: 50% with broncioectases and bronchiolectasis
SLE - Chronic interstitial pneumonia • Radiographic - 6– 24% • HRCT – 24/34 abnormal 11/34 CIP Fenlon HM, Doran M, Sant SM, et al. Am J Roentgenol 1996; 166: 301– 7. Estes D, Christian CL. Medicine (Baltimore) 1971; 50: 85– 95. Raynaud’s phenomenon, swollen fingers, sclerodactyly, telangiectasia, dyspnoea, nailfold capillary abnormalities May be efficacious: Corticosteroids Immunosuppressive agents
与ILD的相关因素 l l 与病种有关 在RA中与RF的滴度有关 DM/PM与抗Jo-1抗体有关 抗RNP抗体 Clin Exp Allergy 2003; 33: 226 ~ 232 Arthritis Rheum 2002; 47: 614 ~ 622
治疗 l ILD 治疗的中心问题是GC和免疫抑制的指征 GC是最常用药,众多病人无反应 预后取决于分型 GC+CTX疗效好于单用GC Am J Respir Crit Care Med 1996; 154: 400 Arthritis Rheum 1994; 37: 1290 Semin Arthritis Rheum 2003; 32: 273
治疗 l ILD 治疗的中心问题是GC和免疫抑制的指征 GC是最常用药,众多病人无反应 预后取决于分型 GC+CTX疗效好于单用GC Am J Respir Crit Care Med 1996; 154: 400 Arthritis Rheum 1994; 37: 1290 Semin Arthritis Rheum 2003; 32: 273
治疗RA-ILD CTX, cyclosporine , azathioprine, hydroxychloroquine have all been reported to be useful in the management of RAassociated ILD refractory to corticosteroids.
治疗RA-ILD TNFa? l. In a preliminary study, infliximab also led to stabilization or improvement in symptoms, lung function, and radiology scores in five RA-ILD. RCT trial needed l非UIP--recommend corticosteroids UIP--recommend TNFa screen for secondary PH. l. Bosentan?
治疗SSc-ILD prognosis better --77. 5% respond to IS histopathologic subset severity of disease at presentation increased level of plasma homocysteine PH BAL eosinophil and neutrophil levels? TGFbeta, MMP
the first positive results of a PCT
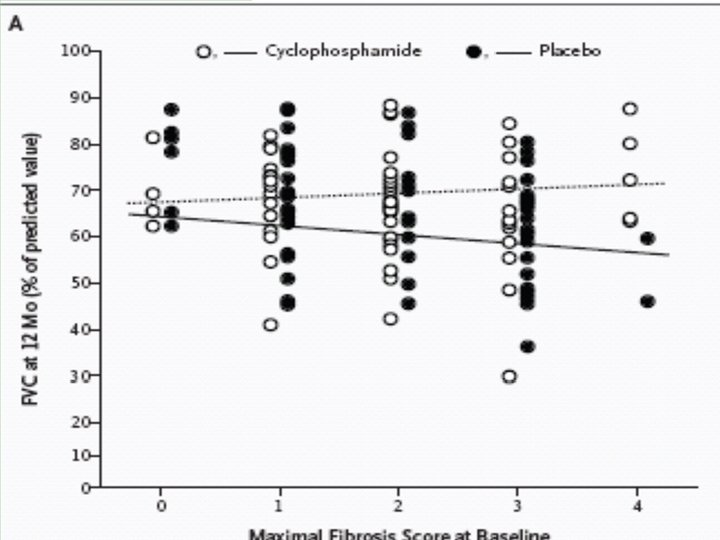
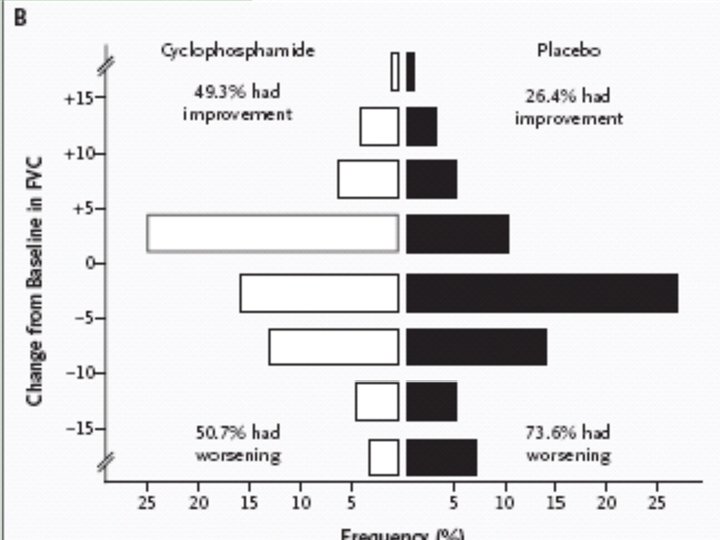
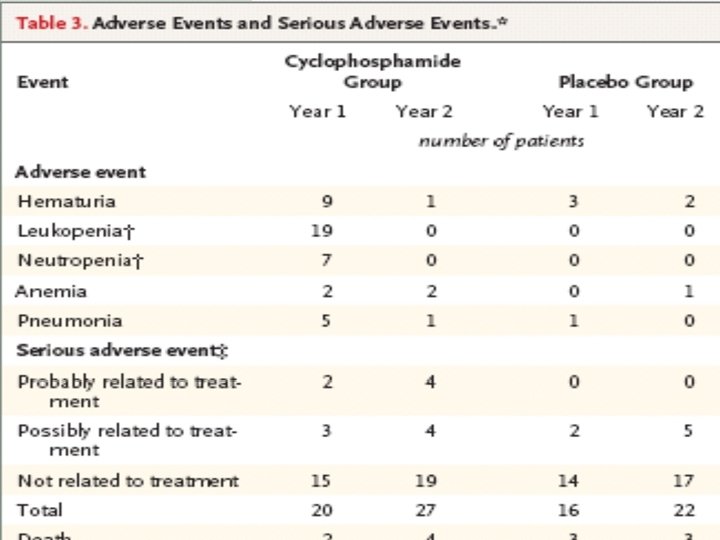
治疗SSc-ILD-NEJM报道 Of 158 patients, 145 completed at least six months of treatment and were included in the analysis. ØThe mean absolute difference in adjusted 12 month FVC% predicted between the CTX and placebo groups was 2. 53% (95%CI 0. 28 to 4. 79%), favoring CTX (P<0. 03).
治疗SSc-ILD-NEJM报道 ØThere were also treatment-related differences in physiological and symptom outcomes, and the difference in FVC was maintained at 24 months. ØThere was a greater frequency of adverse events in the CTX group, but the difference not significant.
治疗SSc-ILD-NEJM结论 ØOne year of oral CTX in symptomatic SSc. ILD had a significant but modest beneficial effect on lung function, dyspnea, thickening of the skin, and the health-related quality of life. ØThe effects on lung function were maintained through the 24 ms of the study.
治疗SSc-ILD-NEJM问题 no significant treatment-related difference was noted in the DLco
治疗ILD-排除感染 l l mimic ILD or develop as a complication of immunosuppressive therapy. Pneumocystis carinii pneumonia. SLE, myositis, WG—chronic corticosteroids, MTX, inhibitors of TNFa all patients with CTD on chronic immunosuppression (>8 ws) should be considered for P. carinii prophylaxis?
治疗ILD-MTX? l l acute hypersensitivity pneumonitis and pulmonary fibrosis May predispose to P. carinii independently of corticosteroid use prefer to avoid using MTX in patients with ILD recent studies suggest that low-dose MTX is associated with a very low risk of pulmonary toxicity, suggesting that patients should not be automatically discontinued from the MTX, provided that the ILD does not progress
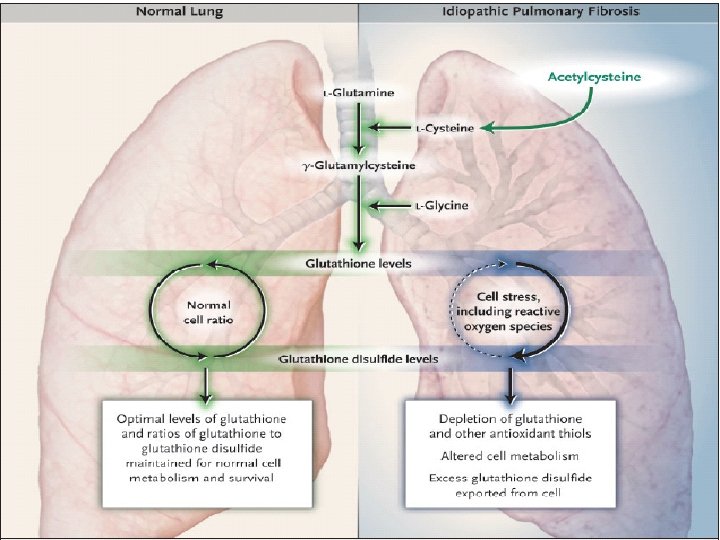
治疗-IPF启示 Ø Ø Ø The synthesis of glutathione can be accelerated by the administration of NAC, which crosses cell membranes easily and can be converted to l-cysteine. Uptake of l-cysteine is an important ratelimiting step for the synthesis of glutathione. NAC increases the pool of other antioxidant thiols that also protect cells from injury.
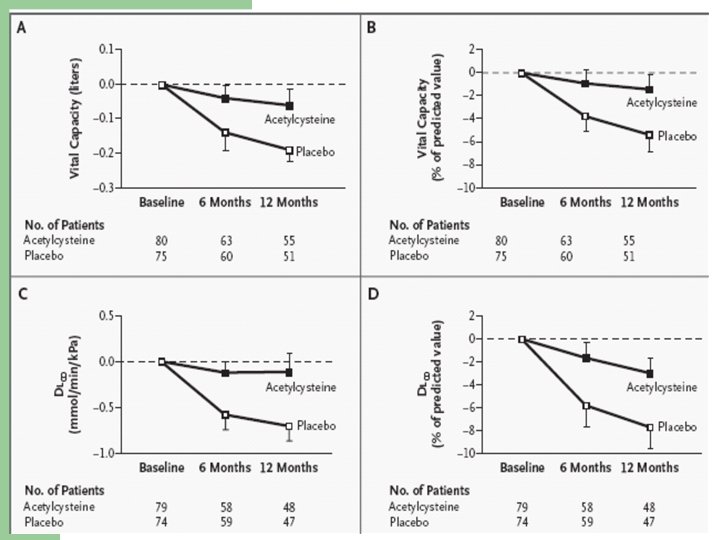
l l 182 patients (92 to NAC and 90 to placebo). 155 (80 NAC and 75 placebo) had UIP, as confirmed by HRCT and histologic findings reviewed by expert committees, and did not withdraw consent before the start of treatment.
l l 57/80 taking NAC (71%) and 51/75 taking placebo (68%) completed one year of treatment. NAC slowed the deterioration of VCand Dlco at 12 months, absolute differences in the change from baseline between patients taking NAC and those taking placebo were 0. 18 liter (95%CI, 0. 03 to 0. 32), relative difference of 9% , for VC(P=0. 02), and 0. 75 mmol per minute per kilopascal (95%CI, 0. 27 to 1. 23), or 24%, for Dlco(P=0. 003).
l l Mortality during the study was 9 %NAC and 11 %placebo(P=0. 69). There were no significant differences in the type or severity of adverse events between patients taking NAC and those taking placebo, except for a significantly lower rate of myelotoxic effects in the group taking NAC (P=0. 03).