l l l l Lord Buddha623 543 Socrates469
 哲學家蘇格拉底 (Socrates,西元前469 -399年 ) 亞歷山大大帝(Alexander")
歷史上的癲癇名人 l l l l 佛陀 (Lord Buddha,西元前623 -543) 哲學家蘇格拉底 (Socrates,西元前469 -399年 ) 亞歷山大大帝(Alexander the Great,西元前356 -323 ) 羅馬凱撒大帝(Julius Caesar,西元前100 -44) 詩人但丁(Dante Alighieri, 1265 -1321) 俄羅斯沙皇彼得大帝(Peter the Great ,西元1682 -1725) 作曲家韓德爾(George Frederick Handel,西元1685 -1759) 法蘭西皇帝拿破崙(Napoleon Bonaparte,西元1769 -1821) 詩人拜倫(Lord Byron,西元1788 -1824) 教宗比約九世(Pius IX ,西元1792 -1878) 柴可夫斯基(Pyotr Ilyich Tchaikovsky,西元1840 -1893) 諾貝爾(Alfred Nobel,西元 1833~1896) 畫家文生梵谷(Vincent van Gogh ,西元1853 -1890)

定義 l l l l Seizure: the clinical manifestation of an abnormal, excessive, and hypersynchronous discharge of a population of cortical neurons. Epilepsy: a disorder of the CNS characterized by recurrent seizures unprovoked by systemic or neurologic insults. Epileptic syndrome: a particular form of epilepsy, often implying specific causes, clinical manifestations, and prognosis Aura: the earliest part of a seizure, and typically the only part recalled by the patient after consciousness is lost. Postictal period: time between the end of the seizure and recovery to the baseline state. Status epilepticus: 30 or more minutes of continuous or recurrent seizures without recovery to baseline function. Symptomatic seizure: a seizure that results directly from an neurologic or systemic insult Antiepileptic drug (AED): a medication given to prevent or suppress seizures
 l Classification of Epileptic Seizures in 1981 l Classification")
International League Against Epilepsy (ILAE) l Classification of Epileptic Seizures in 1981 l Classification of Epilepsies and Epileptic Syndromes in 1989 l *Semiological Seizure Classification in 1998 l A Proposed Diagnostic Scheme for People with Epileptic Seizures and with Epilepsy in 2001 http: //www. ilae-epilepsy. org/
")
Classification of Epileptic Seizures (1981)
 l Localization-Related (Local, Focal, Partial) Epilepsies and")
Classification of Epilepsies and Epileptic Syndromes (1989) l Localization-Related (Local, Focal, Partial) Epilepsies and Syndromes ¡ ¡ ¡ l Idiopathic (with age-related onset) Symptomatic Cryptogenic Generalized Epilepsies and Syndromes ¡ ¡ ¡ Idiopathic (with age-related onset) Cryptogenic or Symptomatic Epilepsies and Syndromes Undetermined Whether Focal or Generalized l Special Syndromes l ¡ Situation-related seizures
")
Semiological Seizure Classification (1998)
 A seizure type is determined by the")
ILAE Proposed Seizure and Epilepsy Classification (2001) A seizure type is determined by the patient’s behavior and EEG pattern during the ictal event l New system emphasizes semiology and etiology of behavior during seizure l It consists of 5 levels or axes organized to facilitate logical clinical approach l Diagnostic studies ¡ Therapeutic strategies ¡ l Currently being evaluated ILAE: International League Against Epilepsy. Engel J Jr, et al. Epilepsia. 2001; 42(6): 796 -803.

2001 ILAE Proposed Diagnostic Scheme l Axis 1: Ictal phenomenology l Axis 2: Seizure type l Axis 3: Syndrome (from list of Epilepsy Syndromes) l Axis 4: Etiology l Axis 5: Impairment

Incidence of Acute Symptomatic and Unprovoked Seizures by Age Incidence/100, 000 300 Acute Symptomatic* Unprovoked† 250 200 150 100 50 0 0 20 40 Age (yrs) *Annegers JF, et al. Epilepsia. 1995; 36: 327 -333. †Hauser WA, et al. Epilepsia. 1993; 34: 453 -468. 60 80

致死率 在年輕成人族群,死亡率是同年齡層的三倍 l 統計上,平均減少壽命可高達 18年 l 死亡與下列情形有關 l ¡ ¡ ¡ An underlying brain disease, such as a tumor or infection; Seizures in dangerous circumstances, leading to drowning, burns or head injury, for example; Status epilepticus; Sudden and unexplained causes, or a possible respiratory or cardio-respiratory arrest during a seizure; Suicide.

預後 In developed countries, more than 60% of patients achieve long-term remission, usually within 5 years of diagnosis. l Predictors of good outcome include earlier age of onset, fewer early seizures, and early response to drug treatment. l Up to a third of people having seizures develop chronic epilepsy. l People with chronic epilepsy also have an increased risk of comorbid conditions, including cardiovascular and cerebrovascular disorders, gastro intestinal disorders, fractures, pneumonia, chronic lung diseases, and diabetes. l

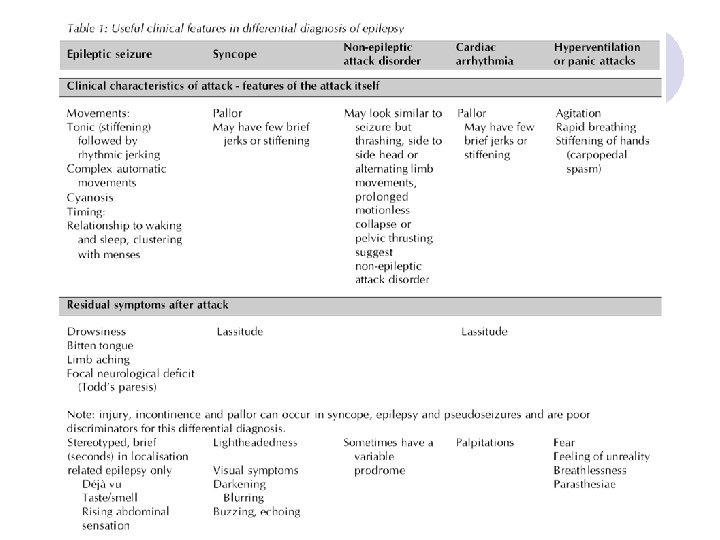
Diagnosis of Epilepsy l Clinical history is key ¡ Experience at onset ¡ Report of observers ¡ Postictal experiences l Electroencephalogram ¡ Generalized syndrome: commonly abnormal ¡ Partial seizures: rarely abnormal on first recording l Imaging study: MRI

Diagnosis --- History l Drug treatment history ¡ ¡ ¡ l Medical history ¡ ¡ l l Current and previous AEDs Epileptogenic drugs (eg, ciprofloxacin, tramadol, antimalarials) Drugs with AED interactions (eg, warfarin, digoxin, oral pills) blackout events, absences, myoclonus, or photosensitivity. Potential cerebral insults, (eg, premature and/or traumatic birth, febrile seizures, CNS infection, and head injury) Heart disease Depression and anxiety commonly accompany epilepsy, but significant psychiatric history (including misuse and illicit drug dependence) might favour psychogenic seizures. Family history Social history ¡ education, employment, driving status, family planning, home situation, sporting interests, use of alcohol and illicit drugs.

Signs and Symptoms Suggestive of a Seizure Drowsiness and confusion following the event Stereotypical motor activity Loss of memory for the event Physical trauma, especially oral lacerations Bladder or bowel incontinence Muscle aches and pains Distortions in sensations including olfactory, gustatory, auditory, visual, and tactile l Positive family history l History of head trauma or other CNS pathology l l l l
, dysmorphic features, body size")
Diagnosis --- Physical Examination Epilepsy: skin stigmata (neurofibromatosis, tuberous sclerosis), dysmorphic features, body size asymmetry (eg, nail size), and cerebral bruit. l Long term AEDs may result in tremor, hair loss, weight gain (eg, sodium valproate, gabapentin), gum hypertrophy, hirsutism, acne, ataxia, or absent reflexes (eg, phenytoin). l Probable syncope: cardiovascular examination is essential, particularly in the elderly patient. l It can be helpful to provoke the physical symptoms of hyperventilation by deep breathing for three minutes. Hyperventilation may also induce typical absences in children. l
 hyperplasia occuring in approximately 20% of patients.")
Medication l Phenytoin ¡ Gingival (Dilantin) hyperplasia occuring in approximately 20% of patients.
 ¡ Thrombocytopenia")
Medication l Valproate (Depakote) ¡ Thrombocytopenia

Diagnosis --- EEG l l l A normal EEG does not exclude a diagnosis of epilepsy. EEG can be used for the diagnosis in patients in whom the clinical history indicates a significant probability of epilepsy. A single routine EEG will show definite epileptiform abnormalities in 29 -38% of adults who have epilepsy. With repeat recordings this rises to 69 -77%. The sensitivity is improved by performing an EEG soon after a seizure, and by recordings with sleep or following sleep deprivation. Incidental epileptiform abnormalities are found in 0. 5% of healthy young adults. EEG should be used to support the classification of epileptic seizures and epilepsy syndromes when there is clinical doubt. EEG should be performed in young with generalised seizures to aid classification and to detect a photoparoxysmal response.

Diagnosis --- Brain Imaging l l l Brain imaging detects lesions in 21 -37% of patients presenting with epilepsy, their detection may have implications for future management should the epilepsy become intractable. MRI is the modality of choice in patients with epilepsy. Brain imaging is not routinely required when there is a confident diagnosis of an idiopathic generalised epilepsy and if there is rapid and complete response to the first line antiepileptic drug. CT has a role in the urgent assessment of seizures, or when MRI is contraindicated. MRI carried out for the assessment of drug-resistant epilepsy requires specialised protocols and expertise (eg to detect hippocampal sclerosis).

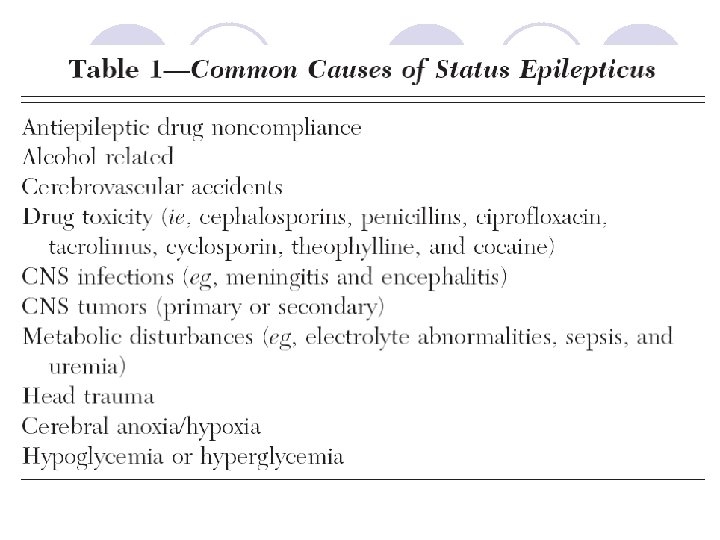
Metabolic Etiologies of Seizures l l l Hypoglycemia Hyponatremia Hypocalcemia Hypomagnesemia Hepatic failure Renal failure, uremia Anoxia/hypoxia Drug/toxin Medication-induced Nonketotic hyperglycemia Inborn errors of metabolism Thyroid storm
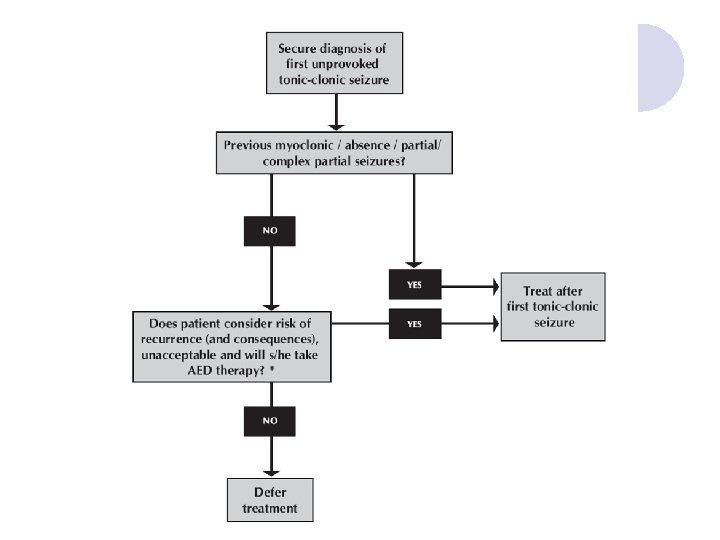

Risk of Recurrence After First Seizure l Overall risk 30 -40% ¡ ¡ l Risk of recurrent epileptic seizures ¡ ¡ ¡ l risk highest soon after seizure: up to 80% after a week >80% risk if EEG shows epileptic discharges >90% risk if patient has tumour/neurological deficit <40% risk if seizures are acute symptomatic sudden unexplained death accidents extended driving licence withdrawal Risk of AED therapy ¡ ¡ ¡ side effects - minor 20 -30%, life-threatening very rare drug interactions eg oral pills, with AEDs teratogenesis (4 -6% major malformation with one AED)

Treat a Single Seizure Largely decided by the risk of further seizures Overall the risk is 30 -40%; this is greatest in the first twelve months and falls to <10% after two years. l AEDs should be offered after a first tonic-clonic seizure if: l l ¡ ¡ The patient has had previous myoclonic, absence or partial seizures EEG shows unequivocal epileptic discharges The patient has a congenital neurological deficit The patient considers the risk of recurrence unacceptable.

Evaluating Recurrent Seizures l Inadequate serum drug levels and patient compliance ¡ Check serum levels and also check for appropriate dose Addition of other medications which may adverely influence anti-epileptic drug metabolism l Ongoing infection l ¡ ¡ l CNS infection Systemic infection/fever Metabolic and/or electrolyte disturbances ¡ ¡ ¡ Hyponatremia, especially in patients on carbemazepine Hypocalcemia Hypoglycemia, especially in diabetics Progression of previously documented disease, especially neoplastic processes l Alcohol or drug ingestion or withdrawl l Heightened stress or anxiety l Sleep deprivation l
 Phenytoin")
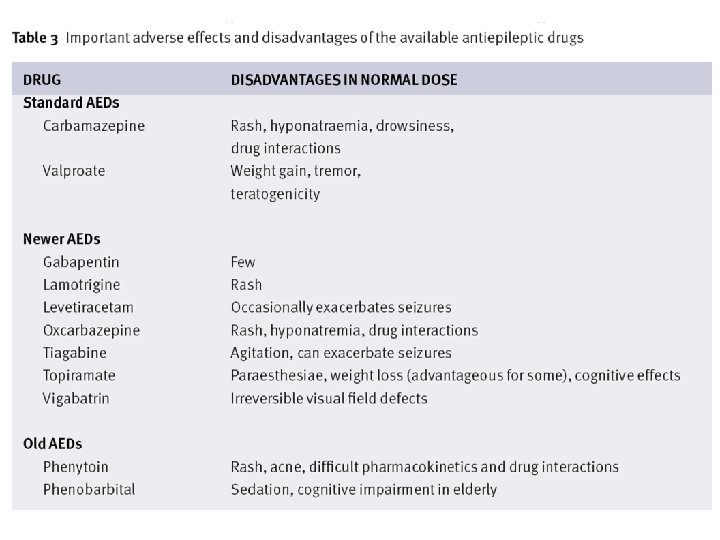
Classic Versus Newer Anticonvulsants Classic AEDs l l l l l Phenobarbital (1912) Phenytoin (Dilantin® 1938) Primidone (Mysoline® 1952) Acetazolamide (Diamox® 1952) Ethosuximide (1953) Carbamazepine (Tegretol® 1963) Diazepam (1965) Valproic acid (Depakine® 1968) Clonazepam (Rivotril® 1975) Newer AEDs l l l Vigabatrin (Gabitril® 1989) Lamotrigine (Lamictal® 1991) Gabapentin (Neurontin® 1993) Topiramate (Topamax® 1995) Levetiracetam (Keppra® 1999)

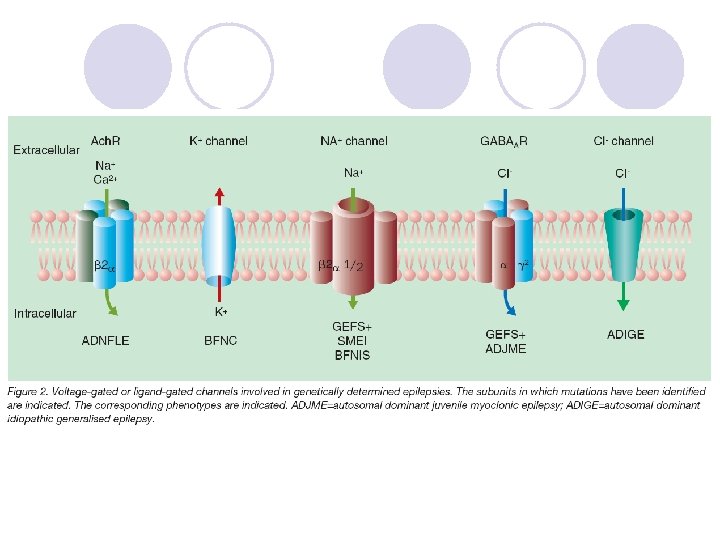
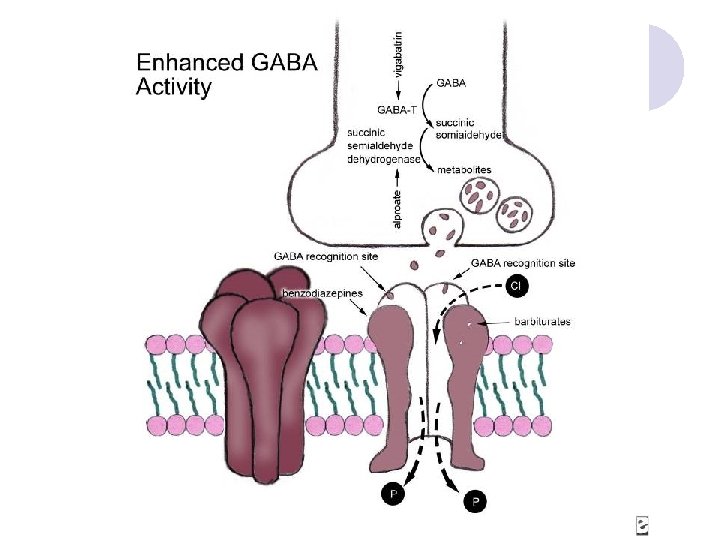
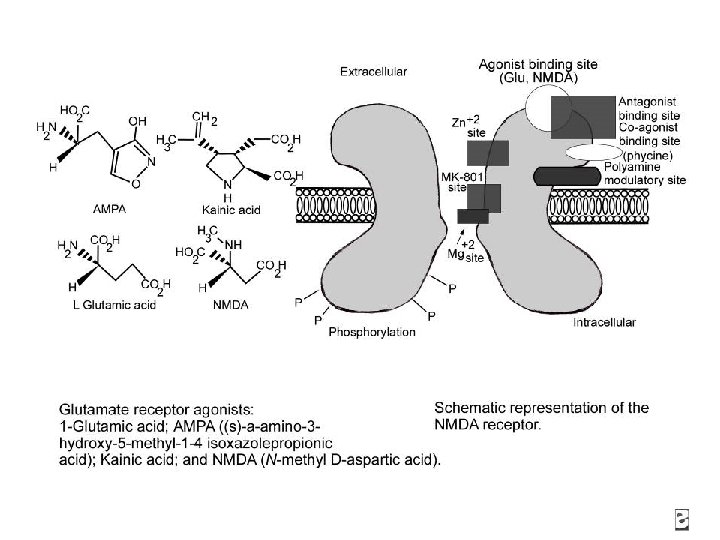
Anticonvulsants: Mechanisms of Action Ligand-gated ion channel in neuronal membrane NH 2 COOH
 Voltage-gated sodium channel Open Inactivated Na+ A A")
Anticonvulsants: Mechanisms of Action (cont. ) Voltage-gated sodium channel Open Inactivated Na+ A A I Na+ Carbamazepine Phenytoin A = activation gate I = inactivation gate Mc. Namara JO. Goodman & Gilman’s. 9 th ed. 1996: 461 -486. I Na+ Lamotrigine Valproate
 Voltage-gated calcium channel Ca 2+ Valproate Ca 2+")
Anticonvulsants: Mechanisms of Action (cont. ) Voltage-gated calcium channel Ca 2+ Valproate Ca 2+ Subtypes L-type T-type N-type P-type Ca 2+ Mc. Namara JO. Goodman & Gilman’s. 9 th ed. 1996: 461 -486. Ca 2+ Dimethadione Ethosuximide

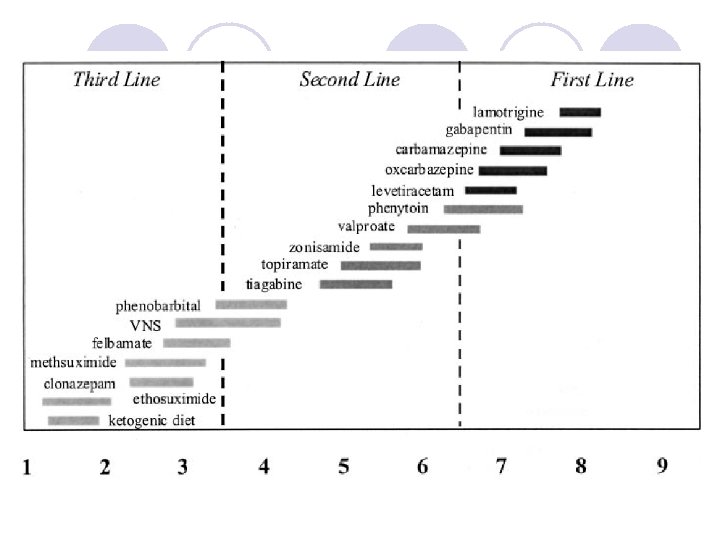
AED Choice by Seizure Type Partial Simple Complex Secondary generalized Generalized Tonicclonic Tonic Myoclonic PHT, CBZ, PB, GBP, TGB, LVT, OCBZ Atonic Infantile Spasms ACTH TPM? TGB? VGB? VPA, LTG, TPM, (FBM) ZNS Absence ESX
: 3# qd(I), 1#/2 -4 W(E), 36#/D(M)")
Dosages of AEDs l l l Phenytoin (100): 3# qd(I), 1#/2 -4 W(E), 36#/D(M) Carbamazepine(200): 1# bid(I), 1#/W(E), 2 -3# bid(M) Valproate(500): 1# bid(I), 1#/W(E), 1 -3# bid(M) Gabapentin(400): 1# bid(I), 1#/D(E), 2 -9#/D bid to tid(M) Topiramate(100): 0. 5# qd(I), 0. 5#/W(E), 1 -8# bid(M)
: 1# tid(I), 1#/3 D(E), Max 20 mg/D l Phenobarbital(30):")
Dosages of AEDs Clonazepam(0. 5): 1# tid(I), 1#/3 D(E), Max 20 mg/D l Phenobarbital(30): 2# qd(I), 1#/4 W(E), 3 -4#/D l Lamotrigine(50) l ¡ ¡ ¡ Monotherapy: 0. 5# qd for 2 W, then 1# qd for 2 W; 2 -5# bid(M) Add-on without Valproate: 1# qd for 2 W, then 1# bid for 2 W; 1 -2#/W(E); 3 -5# bid(M) Add-on with Valproate: 0. 25# qd for 2 W, then 0. 5# bid for 2 W; 0. 5 -1#/W(E); 1 -2# bid(M)

Anxiety Ataxia X Cardiac block X CHF trig ine Ox car baz epi To ne pir a Zo mate nis am ide Fe lba ma te La mo ine Tia gab cet ira in vet Le Ga bap ent te roa X am l bit a Va lp Ph en ob ar zep ma rba Ca Ph eny toi n ine AED Adverse Events X XX X X X X 7 X 7 Cognitive impairment X X X Dizziness/diplopia X X XX Duputyren’s contracture Hepatotoxicity Hyponatremia X X XX X X 6 X 8 X 13 X 1 X 9 X = less than 5%; XX = 5% to 15%; XXX = more than 15% X 18 X 22 X X 27

Ph eny toi n Ca rba ma zep Ph ine eno bar bit Va al lpr oat e Ga bap Le entin vet Tia irace gab tam La ine mo trig ine Ox car baz epi To ne pir am ate Zo nis am i Fe lba de ma t Hypotension X Insomnia X Lethargy/sedation X Low WDC X X XX X X X 10 XXX Osteopenia X Thrombocytopenia X 4 X X 28 XX X X 14 X 11 X 15 XXX 3 X 19 Prolonged t 1/2 X 29 X X 5 X 12 X 16 X X 17 X 20 X 21 Renal stones Tremor XX X 23 Weight loss Rash X X X 25 X 30 X 24 XX X = less than 5%; XX = 5% to 15%; XXX = more than 15% X XX X X

bar bit Va al lpr oat e Ga bap Le entin vet Tia irace gab tam La ine mo trig ine Ox car baz epi To ne pir am ate Zo nis am Fe lba ide ma t e Ph eno aze pin rba m n Ca toi eny Ph Aplastic anemia X 11 Weight gain X 19 XX X 26 X 28 X Pancreatitis X = less than 5%; XX = 5% to 15%; XXX = more than 15% 1 2 3 4 5 6 7 8 9 10 11 12 Children under the age of two years are at increased risk Life-threatening 27%, dose-related Thrombocytopenia, leukopenia, granulocytopenia, agranulocytosis, pancytopenia Bullous, exfoliative or purpuric dermatitis, lupus erythematosus, Stevens-Johnson syndrome, toxic epidermal necrolysis Toxic hepatitis, liver damage Arrhythmias, atrioventricular heart block, congestive heart failure, syncope Hepatitis Acute renal failure, renal toxicity, hyponatremia, dilutional, or water intoxication (SIADH) Leukopenia, leukocytosis, eosinophilia, acute intermittent porphyria Aplastic anemia, agranulocytosis, pancytopenia, bone marrow depression, thrombocytopenia Toxic epidermal necrolysis, Stevens-Johnson syndrome, aggravation of disseminated lupus erythematosus 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 Rare Osteopenia or rickets (rare) Agranulocytosis (rare), megaloblastic anemia (rare), thrombocytopenia (rare) Exfoliative dermatitis (rare), Stevens-Johnson syndrome (rare) Hepatic failure (rare), hepatic necrosis (rare) Anemia, eosinophilia, leukopenia, thrombocytopenia Erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis Hepatic failure, hepatitis, pancreatitis Anemia (rare), leukopenia (infrequent) Renal calculi (1. 5%), renal tubular acidosis Stevens-Johnson syndrome (rare), toxic epidermal necrolysis (rare) Aplastic anemia (rare), agranulocytosis (rare) Acute liver failure Agranulocytosis, aplastic anemia, eosinophilia, leukopenia, pancytopenia Bone marrow depression, thrombocytopenia Stevens-Johnson syndrome

INTERACTIONS BETWEEN ANTISEIZURE DRUGS With other antiepileptic Drugs: - Carbamazepine with phenytoin Increased metabolism of carbamazepine phenobarbital Increased metabolism of epoxide. - Phenytoin with primidone Increased conversion to phenobarbital. - Valproic acid with clonazepam May precipitate nonconvulsive status epilepticus phenobarbital Decrease metabolism, increase toxicity. phenytoin Displacement from binding, increase toxicity.

ANTISEIZURE DRUG INTERACTIONS With other drugs: antibiotics anticoagulants cimetidine isoniazid oral contraceptives salicylates theophyline phenytoin, phenobarb, carb. phenytoin and phenobarb met. displaces pheny, v. a. and BDZs toxicity of phenytoin antiepileptics metabolism. displaces phenytoin and v. a. carb and phenytoin may effect.

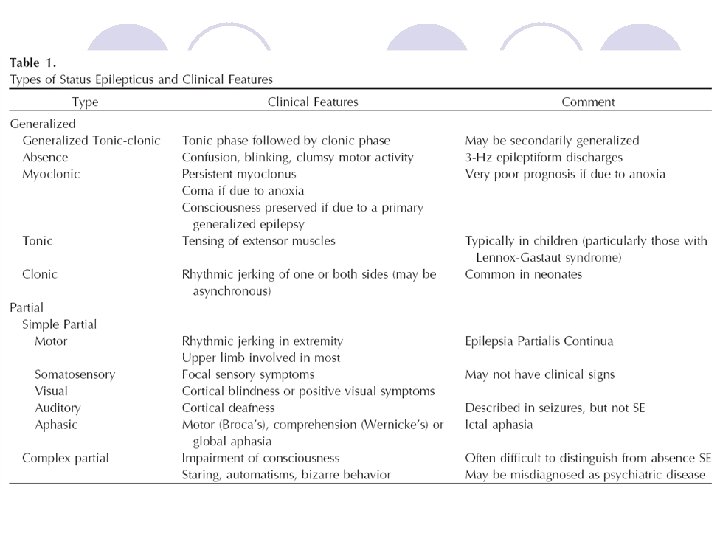
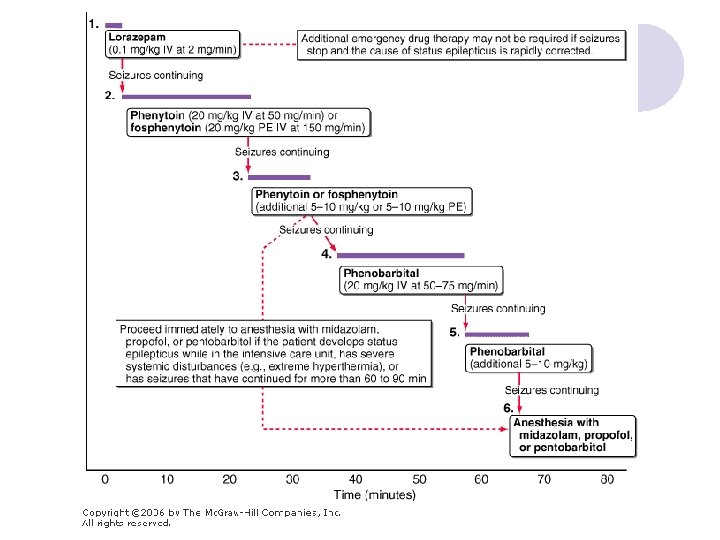
Definitions of Status Epilepticus l. A seizure lasting for more than 30 minutes l Intermittent seizures lasting for more than 30 minutes from which the patient did not regain consciousness International Classifications of Epileptic Seizures
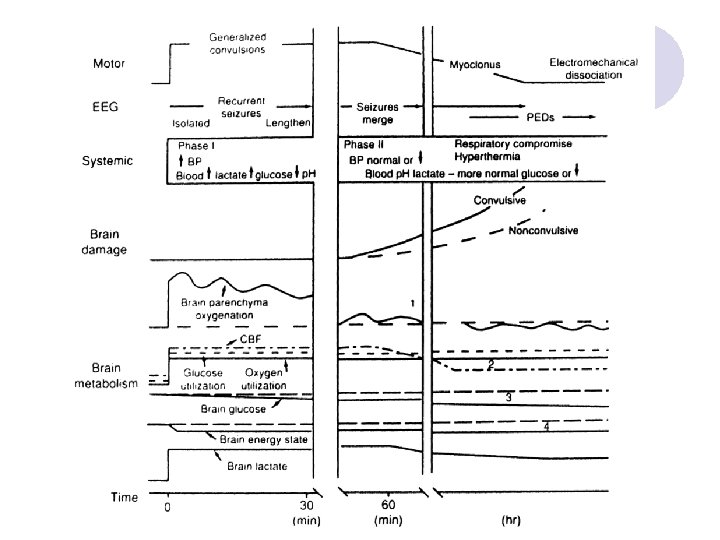

Mortality Rate at 1 month l The most important factor was seizure duration ¡Nonprolonged SE (30 to 59 minutes): 2. 7% ¡Prolonged SE ( > 59 minutes): 32%
 l Phenobarbital (Luminal®) l Propofol (Diprivan®) l Pentobarbital")
維持治療效期之藥物 l Phenytoin (Dilantin®) l Phenobarbital (Luminal®) l Propofol (Diprivan®) l Pentobarbital
 ¡ l Phenytoin")
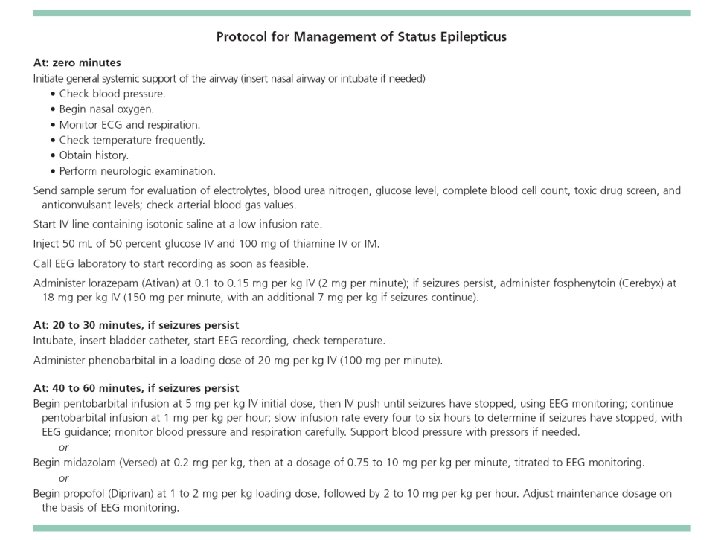
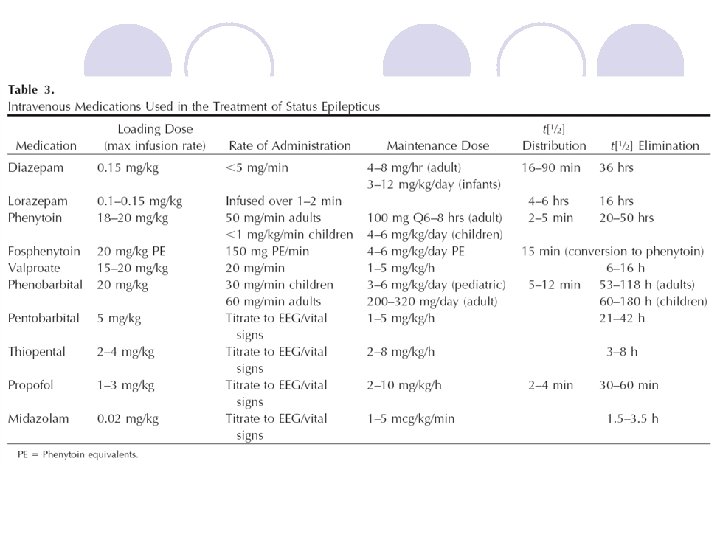
Dosages of AEDs for SE l Diazepam (10 mg/2 ml Amp) ¡ l Phenytoin (250 mg/5 ml Amp) ¡ l ¡ Loading: 0. 2 mg/kg IV; Continuous infusion: 0. 1 -0. 4 mg/kg/h 10 Amp in NS 40 ml IVF keep 5 -25 ml/hr Phenobarbital (100 mg/1 ml Amp) ¡ ¡ l Loading: 15 -20 mg/kg in NS at rate <50 mg/min; Repeat up to 25 -30 mg/kg; MD 100 mg q 6 -8 h Midazolam (5 mg/1 ml Amp) ¡ l 5 -10 mg IV q 10 -20 min; slow IV push <5 mg/min; not to exceed 30 mg/8 h 10 -20 mg/kg IV (NS or D 5 W); infusion rate <100 mg/min In central line Propofol (200 mg/20 ml Amp) ¡ Loading dose: 1 -2 mg/kg IV Maintenance dose: 0. 1 -0. 2 mg/kg/min (6 -12 mg/kg/h) IV

- Slides: 74