KYUNG HEE UNIVERSITY HOSPITAL at GANGDONG PULMONARY THROMBOEMBOLISM

KYUNG HEE UNIVERSITY HOSPITAL at GANGDONG 폐혈관 질환 강동경희대학교병원 호흡기내과 최 천 웅

PULMONARY THROMBOEMBOLISM
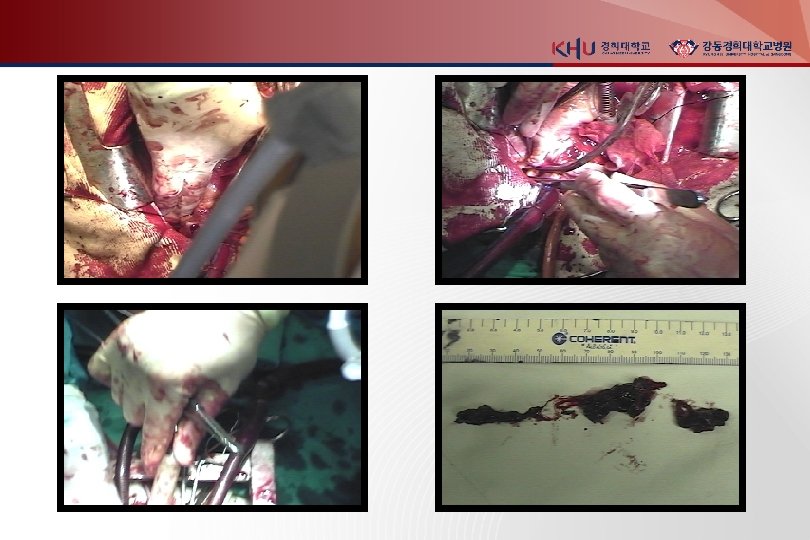
 Rt main pulumonary artery")
Medium sized pulmonary arterty (HE stain) Rt main pulumonary artery

Physiology 1. Increased pulmonary vascular resistance : Pulm a. obst. , vasoactive agent by PLT(serotonin) 2. Impaired gas exchange : increase alveolar dead space 3. Alveolar hyperventilation : stimulation of irritant receptor 4. Increased airway resistance : constriction of distal airway 5. Decreased pulmonary compliance : lung edema, hemorrhage, loss of surfactant

RV dysfunction : usual cause of death pulmonary vascular resistant 증가 RV all tension 상승 RV dilatation & dysfunction diastolic LV impairment underfilling of LV cardiac output & BP 감소 coronary a. perfusion 저하 myocardial ischemia death Rt coronary a. 압박 subendocardial perfusion 감소 myocardial ischemia RV infarction death

Risk factor Predisposed to venous thrombosis 1. Local trauma to the vessel 2. Hypercoagulability 3. Stasis

Stressors precipitate PTE 1. Surgery, trauma 2. Obesity 3. Oral contraceptives, pregnancy, postpartum, postmenopausal HRT 4. Cancer (sometimes occult) or chemotherapy 5. Immobilization (stroke or ICU patients) 6. Indwelling central catheter

Diagnosis Sx and Signs in DVT 1. Cramp in lower calf : most frequent Sx - persists for several days - more uncomfortable as time progresses 2. mild palpation discomfort in lower calf

Diagnosis Sx and Signs in PE 1. Dyspnea : most frequent Sx 2. Tachypnea : most frequent sign 3. Massive PTE : dyspnea, syncope, hypotension, cyanosis 4. Pleuritic pain, cough, hemoptysis : small embolism located distally near pleura 5. Sometimes, a paradoxical bradycardia
,")
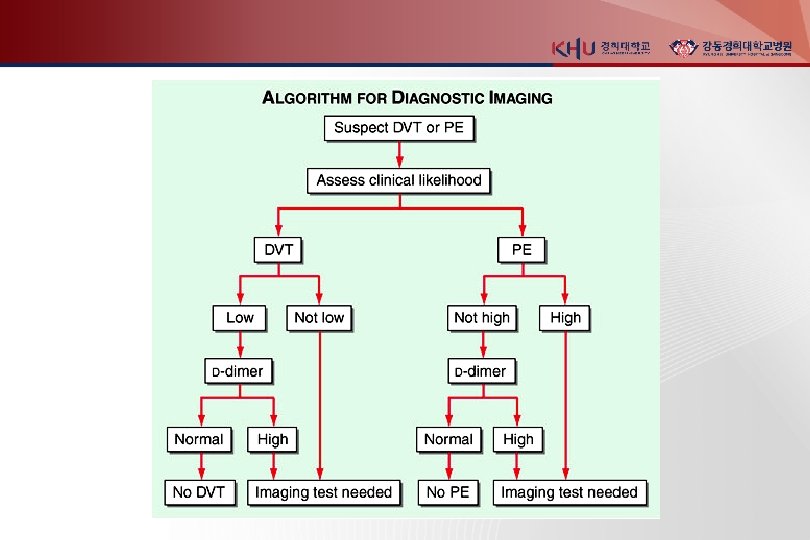
Nonimaging diagnostic modalities 1. Blood tests D-dimer ELISA : sensitive (DVT >80%, PE> 95%), not specific (MI, Pneumonia, sepsis, cancer, postop, preg) “rule-out test” 2. Elevated Cardiac biomarkers - major Complication and mortality Tn-I 증가 : RV microinfarction BNP or NT pro-BNP 증가 : myocardial stretch - predict an increase in major complication & mortality from PE

Nonimaging diagnostic modalities 3. Electrocardiogram : 임상적으로 큰 의미는 없다 sinus tachycardia S in I, Q in V 3, inverted T in V 3 (S 1 Q 3 T 3 sign) T inversion in V 4 -6 : most frequent

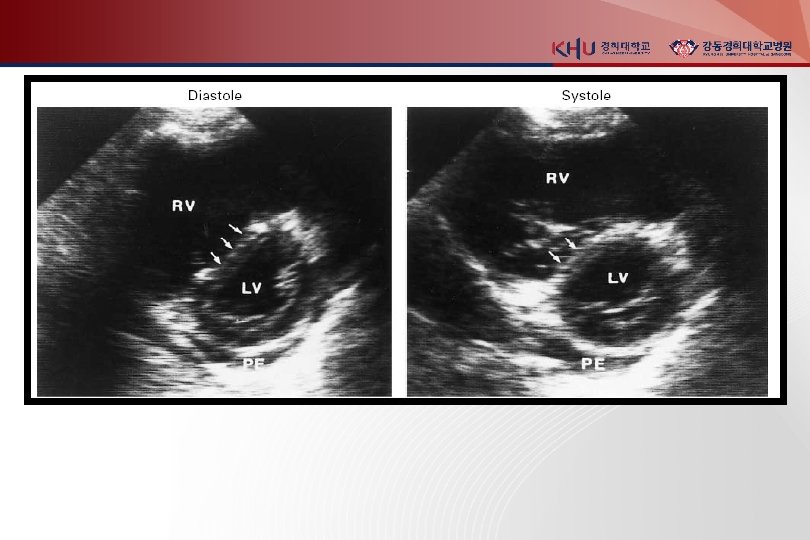
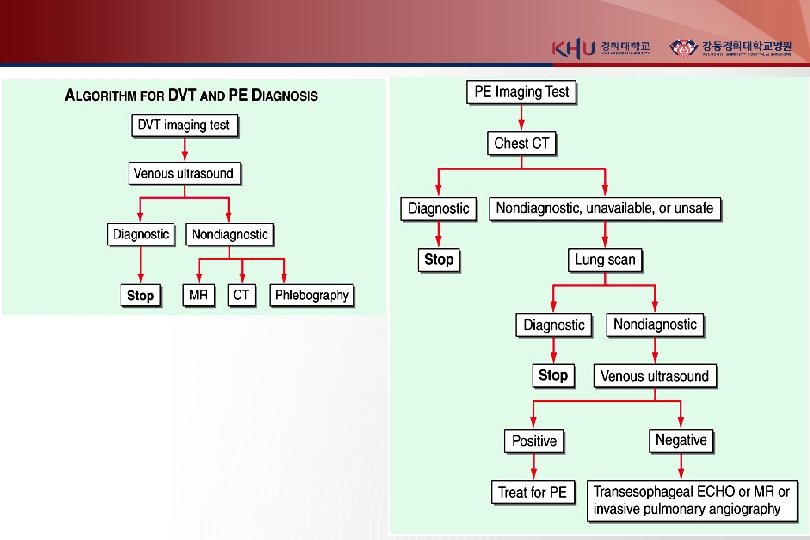
Noninvasive imaging modalities 1. Venous ultrasonography Confirmed DVT loss of “wink” sign 2. Chest X ray : normal or near normal Westermark’s sign (focal oligemia ) Hampton's hump (pph wedged-shaped density above diaphragm) Palla’s sign (enlarged Rt. descending pulmonary artery)
 principle imaging test for Dx. of PTE Multidetector-row spiral CT :")
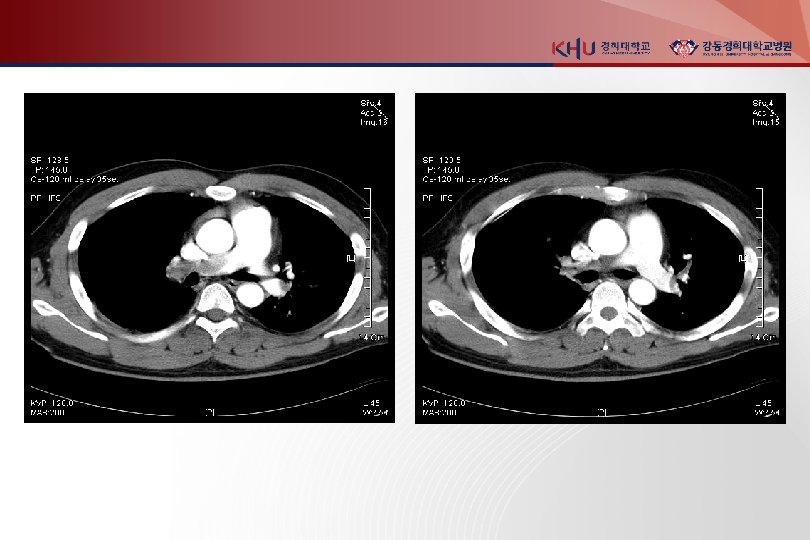
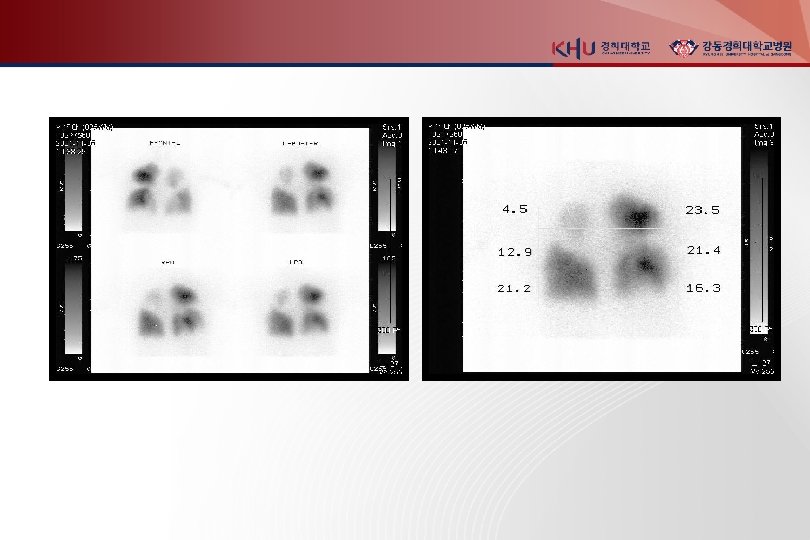
3. Chest CT(enhanced) principle imaging test for Dx. of PTE Multidetector-row spiral CT : small pph emboli RV enlargement : 사망률 5배 증가 다른 폐병변 감별가능 4. Lung scanning second-line test for PTE, 조영제 사용 못하는 환자 high probability : 두개 이상의 segmental perfusion defect 5. Echocardiography for DDx. (AMI, Tampomade, aortic dissection) detection of RV dysfunction

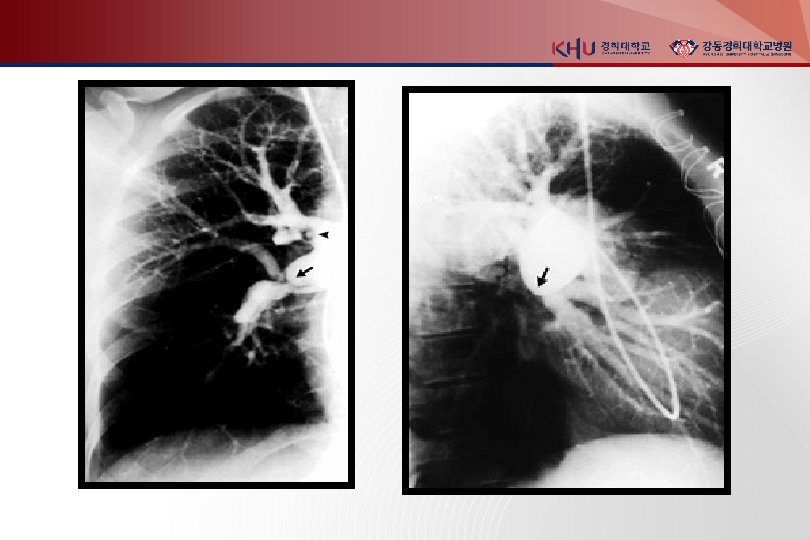
Invasive diagnostic modalities 1. Pulmonary angiograpy 진단 검사로는 chest CT 가 대체 CT 로 충분하지 않거나 intervention이 필요한 경우 시행 (catheter-directed thrombolysis or embolectomy) abrupt occulusion (“cut-off”) of vessels 2. Contrast phlebograpy Venous ultrasonography 가 대체

Nonthrombotic pulmonary embolism 1. Fat embolism : after long bone Fx. , within 3 days unexplained dyspnea, tachypnea, hypoxemia - endothelial injury caused by fatty acid unexplained confusion or cerebral dysfunction sign - direct brain injury, hypoxemia petechiae over upper half of body - reason is not known Tx - supportive Px - mortality <10%

2. Cement and bony fragment embolism : after total hip or knee repacement 3. Amniotic fluid embolism : fetal membrane leak or tear at placental margin 다산부, supportive care 4. Tumor embolism 5. Air embolism

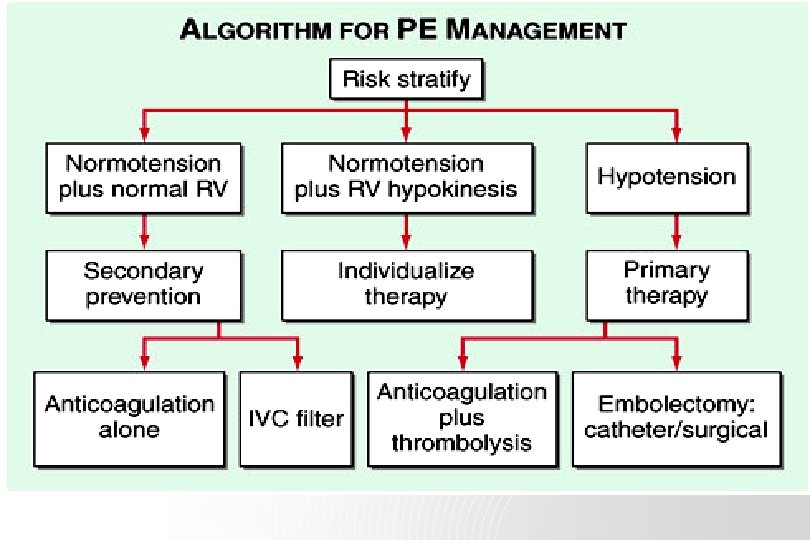
Treatment Primary therapy - high risk of death from Rt heart failure 1. thrombolysis : clot dissolution 2. embolectomy : removal of PTE Secondary prevention of recurrent PE anticoagulation with heparin and warfarin inferior vena caval filter

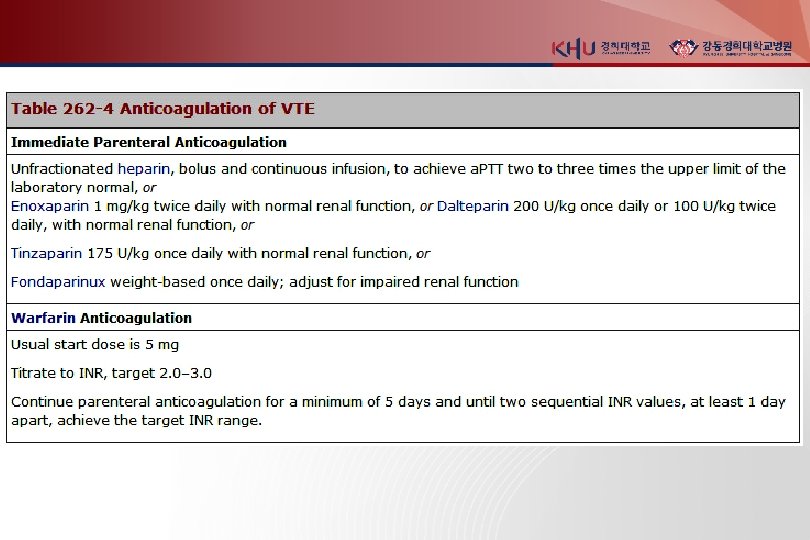
Heparin : 5000 -10000 u bolus 1000 -1500/hr infusion a. PTT는 적어도 2 -3 배 - bind to and accelerate activity of antithrombin III prevents additional thrombus formation permits endogenous fibrinolytic mech. to lyse clot - do not directly dissolve thrombus
 Advantage - short half-life anticoagulant effect abates after several hours - useful in")
1) Advantage - short half-life anticoagulant effect abates after several hours - useful in pt will undergo an invasive procedure (surgical embolectomy) 2) Disadvantage - achieving target a. PTT can be difficult - repeated blood sampling and dose adjustment every 4– 6 h - at risk of developing heparin-induced thrombocytopenia
 Complications - hemorrhage : most important antidote (protamine sulfate) : life threatening or")
3) Complications - hemorrhage : most important antidote (protamine sulfate) : life threatening or intracranial hemorrhage - thrombocytopenia : 50% 이하(<10만) 로 감소하면 stop - osteoporosis - pathologic bone fracture - heparin associated elevation in transaminase levels
 1) less bind to plasma proteins and endothelial cell")
LMWH (low molecular weight heparin) 1) less bind to plasma proteins and endothelial cell 2) greater bioavailability 3) more predictable dose response 4) longer half life 5) not need laboratory monitoring or dose adjustment - Enoxaparin 1 mg/kg bid, tinzaparin 175 units/kg once daily - must be adjusted downward in renal insufficiency
 anti-Xa pentasaccharide 2) administered by once-daily subcutaneous injection 3) no laboratory monitoring")
Fondaparinux 1) anti-Xa pentasaccharide 2) administered by once-daily subcutaneous injection 3) no laboratory monitoring is required 4) <50 kg receive 5 mg, 50– 100 kg receive 7. 5 mg >100 kg receive 10 mg 5) adjust for impaired renal function

Warfarin : initiated in a dose of 5 -10 mg, target INR 2. 5(2. 0 -3. 0) 1) vitamin K antagonist 2) prevents carboxylation activation of factors II, VII, IX, X 3) full effect of warfarin requires at least 5 days 4) Overlapping UFH, LMWH, fondaparinux for at least 5 days - monotherapy during an acute thrombotic illness paradoxical exacerbation of hypercoagulability increase likelihood of thrombosis rather than prevent it
 Complications - bleeding : antidote - Vitamin K, FFP, cryoprecipitate - warfarin induced")
5) Complications - bleeding : antidote - Vitamin K, FFP, cryoprecipitate - warfarin induced skin necrosis - warfarin embryopathy → should be avoided during pregnancy !! (출산 후나 수유 시는 가능)

Duration of Anticoagulation Complications PE following surgery or trauma : low rate of recurrence after 3– 6 months DVT isolated to an upper extremity or calf : by surgery or trauma, 3 months suffices provoked proximal leg DVT or PE : 6 months is sufficient "idiopathic, " unprovoked DVT or PE : recurrence rate is surprisingly high after cessation (VTE that occurs during long-haul air travel is unprovoked) indefinite duration with a target INR between 2. 0 and 3. 0
 active bleeding 2) recurrent venous thrombosis despite intensive anticoagulation")
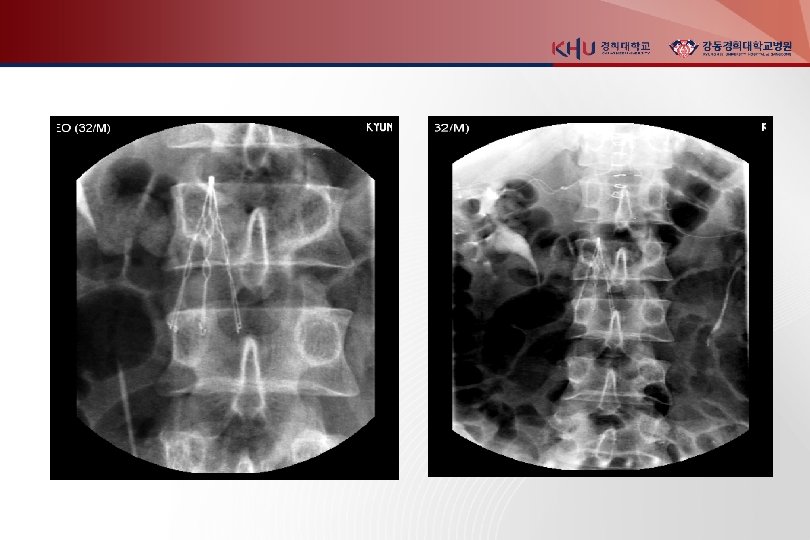
Inferior Vena Caval Filters 1) active bleeding 2) recurrent venous thrombosis despite intensive anticoagulation 3) prevention of recurrent PTE in Rt heart failure (not candidates for thrombolysis) 4) prophylaxis of extremely high risk patients - contraindication to anticoagulation - significant bleeding complications during anticoagulation

Thrombolysis - rapidly reverse Rt. heart failure and lead to lower rate of death and recurrence Indication : Angiographycally proven massive pulmonary embolism with hemodynamic instability Contraindication - Active or recent internal bleeding - Hx. of hemorrhagic stroke - Recent cranial surgery or head injury

Pulmonary Thromboembolectomy - massive pulmonary emboli with 1. Hypotension and end-organ dysfunction despite maximal medical support and 2. Absolute contraindication to thrombolytic therapy or full-dose thrombolytic therapy proved ineffective

Prevention of postphlebitic synrome vascular compression stockings - only therapy to prevent postphlebitic syndrome - daily use of below-knee 30 -40 mm. Hg - halve the rate of developing postphlebitic syndrome - should be prescribed as soon as DVT is diagnosed, should be fitted carefully

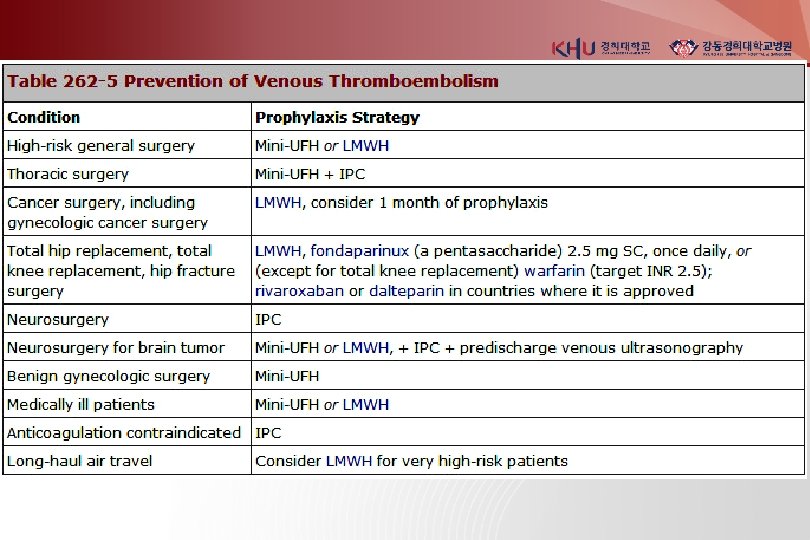
Prevention of VTE GCS graduated compression stockings IPC intermittent Pneumatic compression devices Mini-UFH mini-dose unfractionated heparin (5000 u SC 2 or 3 daily) LMWH low molecular weight heparin (enoxaparin 40 mg once daily) Fondaparinux 2. 5 mg daily

PULMONARY HYPERTENSION

Pulmonary Hypertension - abnormal elevations of pulmonary artery pressure : mean pulmonary artery pressure > 25 mm. Hg at rest > 30 mm. Hg with exercise - results of : left heart failure pulmonary parenchymal or vascular disease thromboembolism combination of these factors

Pathophysiology 원인질환 RV systolic pressure↑ pulmonary vascular resistance↑ chronic change : remodeling of vasculature sustain or promote pulmonary hypertension inadequate RV coronary blood flow to RV myocardium becomes ischemic clinical RV failure poor outcome

Diagnosis Sx & sign : exertional dyspnea – m/c fatigue, angina pectoris, syncope, pph edema : JVP ↑ reduced carotid pulse, palpable RV impulse increased pulmonic component of 2 nd heart sound Rt-sided 4 th heart sound & tricuspid regurgitation pph cyanosis and/or edema - later stages

Diagnosis – Lab. Findings CXR enlarged central pulmonary arteries EKG right axis deviation and RV hypertrophy Echocardiogram commonly demonstrates RV and RA enlargement reduction in LV cavity size TR jet- estimate RV systolic pressure PFT underlying obstructive airways disease hypoxemia and an abnormal DLCO - common features of pulmonary hypertension of many causes

Diagnosis – Lab. Findings HRCT diagnose restrictive lung disease Perfusion lung scan always abnormal in thromboembolic pulmonary hypertension diffuse defects of a nonsegmental nature - long-standing pulmonary hypertension in absence of thromboemboli Laboratory tests include ANA and HIV testing TSH - high frequency of thyroid abnormalities in IPAH
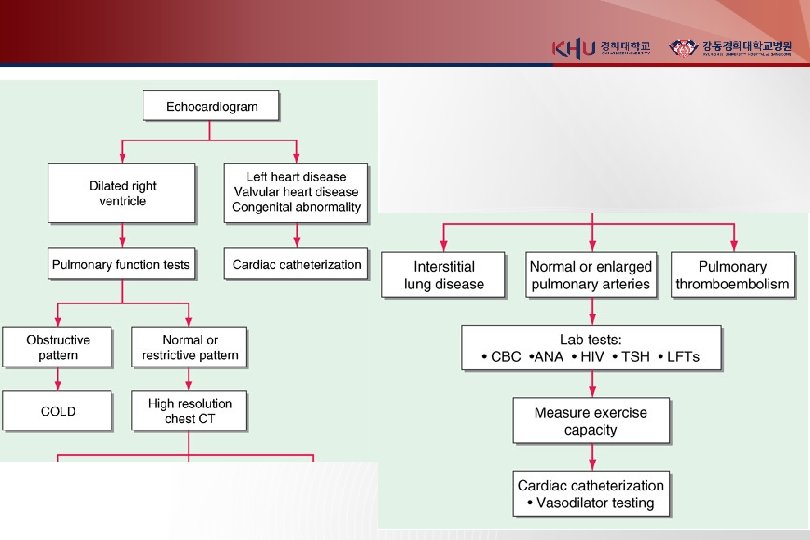

Diagnosis - Cardiac catheterization : accurate measurement of pulmonary artery pressure, cardiac output, and LV filling pressure : exclusion of an underlying cardiac shunt : undergo drug testing with a short-acting pulmonary vasodilator - determine the extent of pulmonary vasodilator reactivity

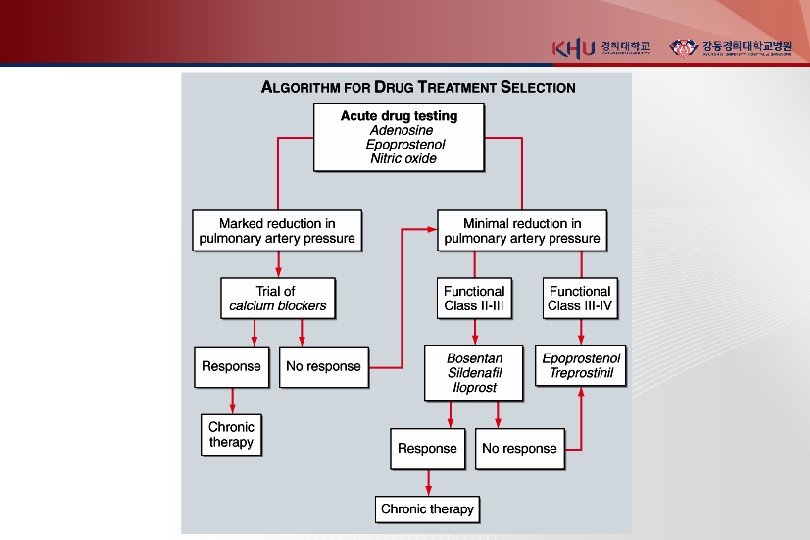
Acute vasodilator test Inhaled nitric oxide - 10– 20 parts per million IV adenosine - 50 ug/kg per min and increased every 2 min until side effects develop IV epoprostenol - 2 ng/kg per min and increased every 30 min until side effects develop responder (fall in m. PAP≥ 10 mm. Hg) : fall in m. PAP ≥ 10 mm. Hg and final m. PAP < 40 mm. Hg treated with calcium channel blockers more favorable prognosis
")
Idiopatic PAH (IPAH)

Incidence 2/100만 Female predominance , 4 th and 5 th decade Familial IPAH : 20% of IPAH - AD - variable age onset - incomplete penetrance

Natural history : uncertain 1. Dyspnea : predominant symptom insidious onset, diagnosed late in its course 2. Mean survival : 2 to 3 years from the time of diagnosis 3. Functional class : strong predictor of survival : class IV < 6 months 4. Cause of death : usually RV failure - progressive hypoxemia, tachycardia, hypotension, edema

Treatment of PAH : cautioned against participating in activities that impose physical stress 1. Diuretics : relieve dyspnea and peripheral edema reducing RV volume overload 2. O 2 supplement : alleviate dyspnea and RV ischemia in pts whose arterial O 2 saturation is reduced 3. Anticoagulation - warfarin, INR 2. 0 -3. 0 - increases survival of patients with PAH

Calcium channel blockers - short-acting vasodilators test 에 반응 있으면 첫 치료약물 - high doses (nifedipine 240 mg/d, amlodipine 20 mg/d) - PAPr 과 pulmonary vascular resistance 드라마틱하게 감소 : 증상호전, regression of RV hypertrophy - improved survival now documented to exceed 20 yrs - 20% 미만의 환자만이 장기적으로 CCB에 반응 - 반응이 없는 환자에게 투여는 금물 : hypotension, hypoxemia, tachycardia, right heart failure 악화 (FDA 승인 안됨)

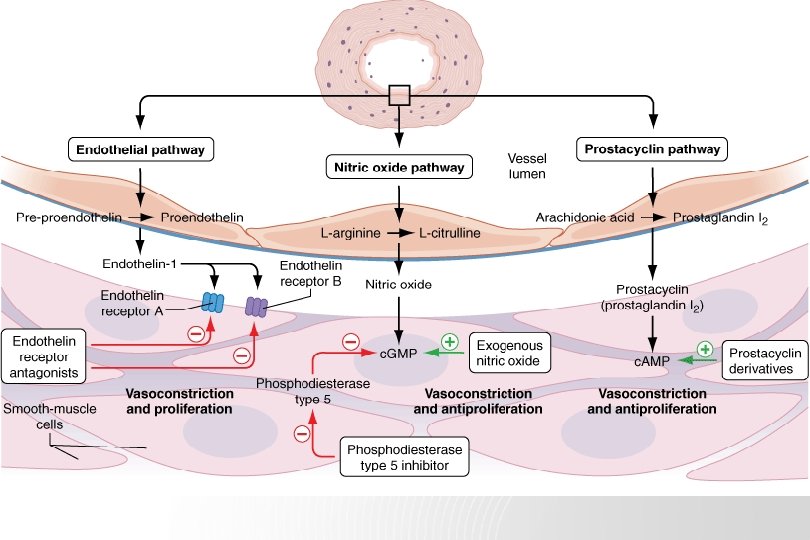
Endothelin Receptor Antagonists Bosentan, Ambrisentan - improved Sx. and exercise tolerance - bosentan : 첫달은 62. 5 mg bid 로 시작, 125 mg bid 까지 증량 - ambrisentan : 5 mg Qd 로 시작하여 10 mg 까지 증량 가능 - 매달 LFT f/u - cyclosporine or glyburide 사용하는 환자는 금기

Phosphodiesterase-5 Inhibitors Sildenafil, Tadalafil - hydrolysis of c. GMP in pulmonary vascular smooth muscle : NO lowers PAPr and inhibits pulmonary vascular growth - improves symptoms and exercise tolerance - sidenafil 20~80 mg tid tadalafil 40 mg Qd - headache : m/c side effect - nitroavasodilators 복용중인 환자는 금기

Prostacyclins Iloprost - prostacyclin analogue - approved via inhalation for NYHA classes III and IV - improve symptoms and exercise tolerance - either 2. 5 or 5 mcg per inhalation treatment : inhaler must be given by a dedicated nebulizer - flushing and cough : m/c side effects - every short half-life (<30 min) : as often as every 2 hrs

Prostacyclins Epoprostenol - NYHA functional class III or IV - improvement in Sx. , exercise tolerance, survival : drug challenge 에 acute hemodynamic response 가 없어도 - IV and permanent central venous catheter : infusion through ambulatory infusion pump system - flushing, jaw pain, and diarrhea : generally tolerated by most patients

Prostacyclins Treprostinil - analogue of epoprostenol - NYHA functional class II - IV - longer half-life than epoprostenol (4 hrs) - stable at room temperature - improvement in symptoms, exercise tolerance - IV or SC through a small infusion pump : local pain at the infusion site, caused to discontinue therapy - side effect는 epoprostenol과 비슷

Lung Transplantation - IV prostacyclin 치료에도 불구 하고 RV failure가 계속 보이는 환자에서 고려 - Acceptable results : heart-lung, bilateral lung, and single-lung transplant - Donor가 있느냐가 치료선택에 제일 중요

- Slides: 67