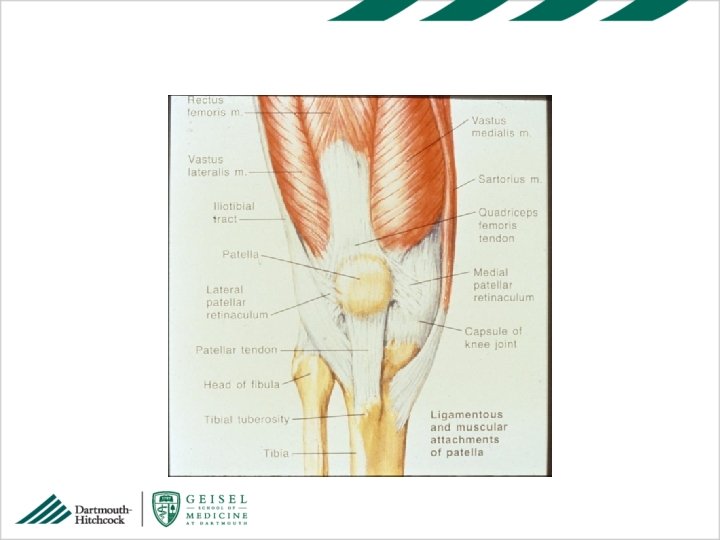
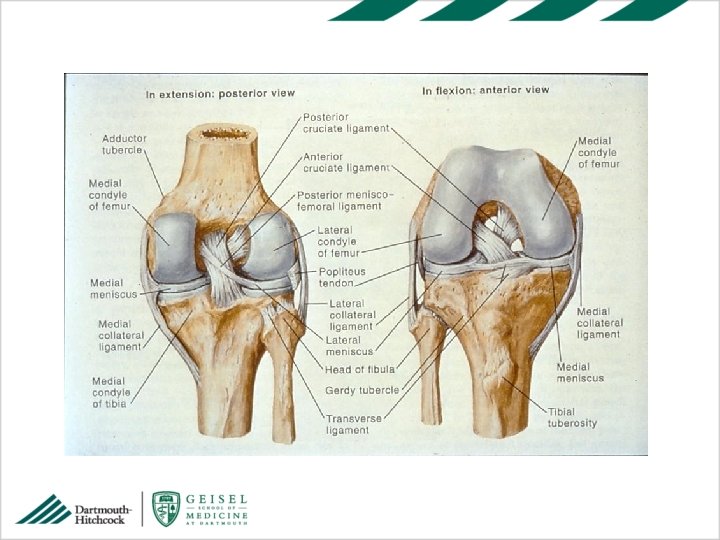
Knee Examination in Context Some Anatomy and History






, anterior Atraumatic Movie goer sign")












- Slides: 22
Knee Examination in Context: Some Anatomy and History Kristine A. Karlson, MD Dartmouth Medical School Community and Family Medicine/ Orthopaedics
Objectives • 1. Recognize key elements of knee injury history and their relation to the physical exam. • 2. Describe common pathologies of knee injuries seen in the outpatient setting and their hallmark physical exam findings. • 3. Perform a focused knee exam.
Knee Pain in Primary Care • Very common cause for office visits • Overuse vs acute injury mechanism • Either could present to the primary care office • Sports/occupational/ accidental mechanisms • So let’s talk about the context first (anatomy, history), and some common approaches to treatment, then go on to the physical exam
Case what’s your diagnosis? A 23 y. o. softball catcher in a recreational league began to notice bilateral anterior knee pain early in the season. She has not injured her knees that she can recall, but several times they nearly gave way. Her pain is worse on long car rides and after playing. There is only occasional mild swelling.
Patellofemoral Pain ■ A common overuse sports injury in women ■ Very common reason for non-injury knee pain visits ■ Characterized by anterior knee pain ■ Patellar subluxation possible (don’t be fooled) ■ History alone often diagnostic ■ If you’re good at only one thing about the knee history, this should be it
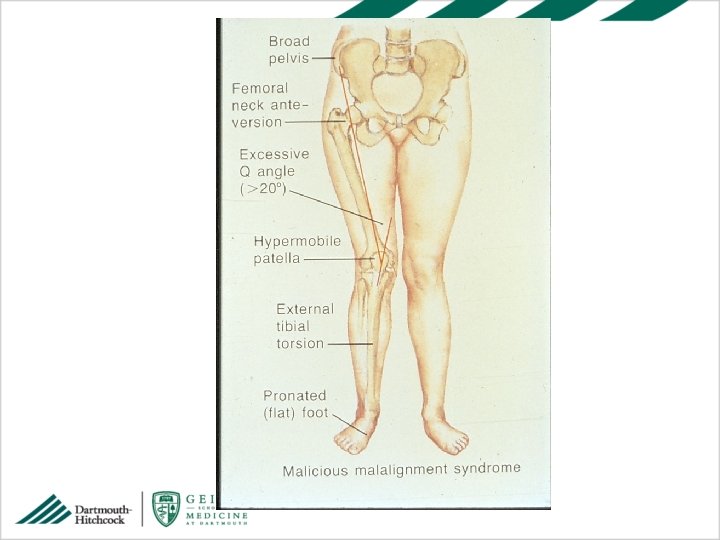
Female predisposition to patellofemoral pain ■ ■ ■ ■ wider pelvis femoral anteversion increased Q angle pronation hypermobile joints relative quad weakness known as the miserable malalignment syndrome, look for all this in your physical
History - Patellofemoral ■ ■ ■ Bilateral (or not), anterior Atraumatic Movie goer sign (pain with sitting, bent knee) Change in usual routine Repetitive flexion and extension May involve subluxation, don’t be fooled
History – MCL Tear • • • Valgus collapse with pop Medial pain Little to no swelling (KEY finding) Sense of medial instability Dislike of full extension Dislike of knees touching each other, rolling over in bed
History – Medial Meniscus Tear • • • Valgus collapse +/- pop Swelling within 24 hrs, often not immediate Locking (truly stuck not transient, brief) Instability or sense of instability
History – ACL Tear • Dramatic injury • Immediate swelling • Unable to bear weight (accompanying bone injury) • Unable to get to full extension when evaluated later
History – Patellar Subluxation/ Dislocation • • • The great mimic Valgus collapse Immediate swelling Inability to bear weight If you’re lucky, they saw the patella dislocated If you’re not, you may be fooled (physical exam really does matter)
Physical Exam Patellofemoral ■ ■ observe for miserable malalignment observe gait for pronation usually no effusion patella for mobility, apprehension, tenderness ■ And examine ligaments and menisci too, even if you’re sure it’s patellofemoral
Finding a Knee Effusion
Physical Exam - Ligaments • Varus/ valgus testing for MCL and LCL • Lachman’s for ACL • Please forget about anterior drawer, low sensitivity/ specificity
Physical Exam - Menisci • • • Full extension standing – do they get there? Squat Bounce in full extension Palpation of joint line Mc. Murray’s Apley’s
Studies ■ plain x-ray 3 or 4 views - AP, lateral, Merchants, notch ■ May not do them all every time, may do none (ie patellofemoral w/o trauma) ■ MRI if suspicious for meniscus, ACL tear, bony injury not seen on plain films ■ ultrasound can evaluate patellar tendon
Treatment - Patellofemoral ■ ■ ice, NSAID active rest/modify activities bracing and taping, orthotics Quadriceps and hip strengthening (refer to PT, not office handout sheets) ■ Reassurance to patient/ parent that this will not lead to arthritis or disability – pain and harm are not the same
Treatment – All Others § Depends on your comfort level with your exam, patient’s short and long term goals, cost considerations, other injuries, etc § In other words “it’s complicated”
Physical Exam in Brief • • • Observe standing ROM, pronation Sit, crepitus, J tracking Lie down, effusion and patellar pain/ mobility MCL, LCL Lachman’s for ACL Palpate joint line, bounce in full extension for meniscus • Mc. Murray’s for meniscus