KNEE EVALUATIONS Anatomy and common injuries The Knee

 ¡ Primarily classified as a")


 Femur (B) Tibia (C, E – tuberosity)")










 ¡ innervates the knee")
")
 Lesser Saphenous Vein (posterior)")




 is the angle formed between a line drawn")
 = The Angle between: 1) ASIS to center of Patella")

























 ¡ Gastro-soleus")













- Slides: 66
KNEE EVALUATIONS Anatomy and common injuries
The Knee Joint n Knee joint proper (tibiofemoral joint) ¡ Primarily classified as a ginglymus (hinge) joint n n n Patellofemoral joint ¡ n n n Sometimes referred to as trochoginglymus (pivotal, screw) joint internal & external rotation occur during flexion Some argue for condyloid (ellipsoid, ovoid)classification arthrodial (gliding) classification (patella on femoral condyles) Femoral condyles articulate with tibial plateaus Tibia - bears most of the weight Fibula – attachment for muscles & ligaments
The Knee Joint n Extends to 180º ¡ n n Hyperextension normal Flexes to 140º With knee flexed 30º or > ¡ ¡ internal rotation 30º occurs external rotation 45º occurs
The Patella n n n Sesamoid bone Imbedded in quadriceps & patella tendon Serves similar to a pulley for improving angle of pull (results in greater mechanical advantage in knee extension)
Surface Anatomy n n n Patella (A) Femur (B) Tibia (C, E – tuberosity) Joint Line (D) Fibula (F) Gerdy’s Tubercle
Internal Knee Anatomy
Internal Knee Anatomy n n n Medial Meniscus Lateral Meniscus Anterior Cruciate Ligament Posterior Cruciate Ligament Articular Cartilage
Ligamentous Anatomy • • Hinged Joint ACL: Ant Stability PCL: Post Stability Lat/Med Stability: LCL/MCL • Menisci: Medial/Lateral
Menisci
Cruciate Ligament Movement
Bursae & Fat Pad of the Knee
Anatomy – Soft Tissue n Quadriceps – ¡ ¡ n Rectus femoris Vastus lateralis Vastus intermedius Vastus medialis (& oblique - VMO) Hamstrings – ¡ Biceps femoris n ¡ ¡ Semitendinosus Semimembranosus n n Inserts primarily on fibula head Inserts posteromedially on medial tibial condyle Popliteal fossa
Muscles n n n Gracilis, Sartorius & Semitendinosus ¡ Common attachment n n n Pes Anscerine Iliotibial Band Gastrocnemius heads – lateral & medial
EXTENSOR MECHANISM ORIGINS: The • Rectus Femoris: AIIS Quadriceps • Vastus Group: Linea Aspera INSERTIONS: • Patellar Retinaculum
FLEXOR MECHANISM The Hamstring COMMON ORIGIN: • Ischial Tuberosity INSERTIONS: • Biceps: Fibular Head • Semimembranosus: Medial Tibial Condyle • Semitendinosus: Pes Anserinus
Nerves n n n Femoral Nerve (L 2, 3, 4) ¡ innervates the knee extensors (quadriceps) ¡ Anterior cutaneous branches of femoral n. Lateral femoral cutaneous N. Saphenous N. – infrapatellar branch
Nerves n Sciatic ¡ tibial division n ¡ semitendinosus, semimembranosus, biceps femoris (long head) common peroneal (fibular) division n biceps femoris (short head)
Vascular Anatomy Femoral Artery & Vein Great Saphenous Vein (medial) Lesser Saphenous Vein (posterior) Popliteal Artery & Vein
Knee Movements
Screw Home Mechanism n Locking mechanism as the knee nears its final extension degrees ¡ n Automatic rotation of the tibia externally (approx. 10 degrees) during the last 20 degrees of knee extension Femoral condyles are a different size ¡ Medial has larger surface area n The tibia glides anteriorly on the femur. As knee extends, the lateral femoral condyle expends its articular distance. The medial articulation continues to glide, resulting in external rotation of the tibia utilizing the lateral meniscus as the pivot point. n ACL & PCL are rotary guides
History n MOI ¡ n n n Position of lower extremity at time of injury (? foot planted, knee extended) Previous history Pain (levels, types, descriptors) Unusual sounds/sensations “pop, clicking, snapping” Chronic vs. acute Location of pain “inside the knee” Surface Shoes Type of activity at time of injury Painful to walk up/down stairs; any clicking, catching Did it swell immediately, slowly? Is the swelling located in the knee or in a pocket?
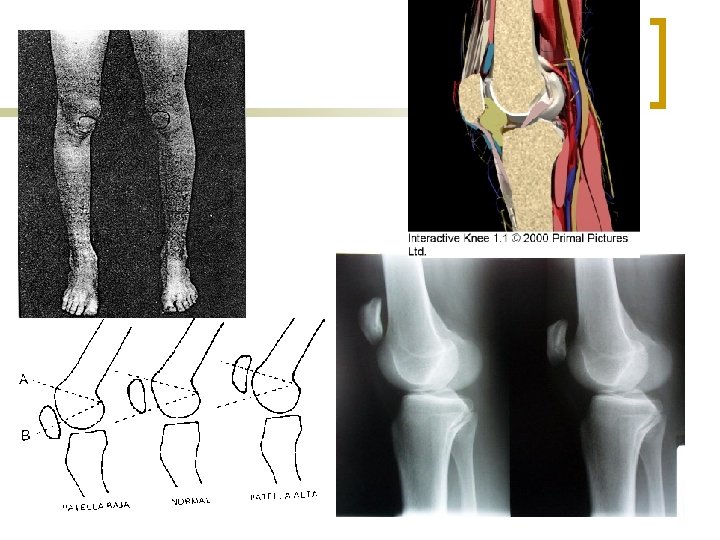
Observation n n n Bilateral comparison Gait (limp, walking on toes, do they not want to extend knee, do they keep the knee stiff) Swelling (girth measurements) Discoloration Deformity (squinting patellae, “Frog-eyed” patellae, Patella alta, Patella baja) Genu valgum, genu varum, recurvatum Musculature – defined/mushy
Q-angle n The quadriceps angle (Q-angle) is the angle formed between a line drawn through the tibial tuberosity and the center of the patella and another line drawn from the anterior superior iliac spine (ASIS) of the pelvis through the center of the patella.
Quadriceps Angle (Q Angle) = The Angle between: 1) ASIS to center of Patella and 2) Patella to Tibial Tubercle NORMAL Men <10° Women <15°
Q-angle n Knee in extension ¡ ¡ n Normal – males 13 degrees Normal - females – 18 degrees Knee in 90 degrees flexion ¡ Both genders – 8 degrees
Palpation n n n n Tibia – tibial plateau, tibial tuberosity, Gerdy’s Tubercle Fibula – head Medial joint line Medial collateral ligament Lateral joint line Lateral collateral ligament “Windows” Medial & Lateral femoral condyles & epicondyles n n n n n Pes anserine tendon Semitendinosus tendon Patella – inferior pole Patellar tendon Quadriceps muscle group Biceps femoris tendon Iliotibial band Popliteal fossa Gastrocnemius heads
Range Of Motion
Stress/Special Tests n On-field vs. Off-field eval ¡ ¡ ¡ Check for fractures, blood, deformities, neurological Valgus Stress Test – MCL Varus Stress Test - LCL Lachman’s – ACL Anterior Drawer – ACL Mc. Murray’s - meniscus
Stress/Special Tests n Check for swelling ¡ n n Check ROM Ely’s Test Check integrity of ligaments & joint stability ¡ n Valgus, Varus, Lachman’s, Anterior/Posterior Drawer, Godfrey’s 90 -90 Test, Posterior Sag Test, Crossover Test, Slocum Drawer Test, External Rotation Test, Pivot Shift Check integrity of meniscus ¡ n Sweep Test, Ballotable Patella Mc. Murray’s, Apley’s Compression/Distraction, Duck Walk, Bounce home Check integrity of patella ¡ Patellar Apprehension, Q Angle, Clarke’s Sign, Patellar glide, tilt, rotation n Check integrity of Iliotibial Band ¡ Ober’s Test, Noble’s Compression Test
Now What? n n n ? Crutches ? Referral ? RICE
Osgood-Schlatter’s Disease
Osgood-Schlatter’s Disease Clinical Features n History ¡ ¡ n Exam ¡ ¡ n young athlete complains of painful enlargement of the tibial tuberosity pain worse with activity, esp. run/jump tender tibial tuberosity tight quads +/- hamstrings Imaging: usually not necessary
Osgood-Schlatter’s Disease Imaging n n n Use in severe or persistent cases to rule out other problems Not used to make the diagnosis in most cases May show fragmentation of the anterior tibial tuberosity
Osgood-Schlatter’s Disease Treatment n n n Relative rest; cross-training Ice Hamstring stretching Strapping of patellar tendon Rare: temporary immobilization Return to play: ¡ Pain-free with sports activity
Osgood Schlatter’s Disease Surgery Indications n Persistent, painful os after growth complete
Housemaid’s knee
Joint Stability Testing n n n MCL: Valgus Load LCL: Varus Load ACL: Lachman, Ant drawer, Pivot Shift n n PCL: Posterior Drawer, Sag sign, Quadriceps Active Postero-lateral complex: Ext Rot
MCL Stability Apply Valgus or Medial Stress Test in 30° flexion LCL Stability Apply Varus or Lateral Stress
Grading collateral ligament injuries n n Grade I: mild; no laxity Grade II: partial tear; laxity w/ firm endpoint Grade III: complete tear; laxity w/o firm endpoint Why does it matter? Prognosis
Treatment of MCL/LCL injuries n Grades I-II ¡ ¡ n knee immobilizer until pain gone ROM/strength ex’s as pain allows Grade III: ¡ ¡ r/o associated injuries knee immobilizer at 30° NWB 3 weeks knee immob 30 -80 ° NWB 4 wks progressive ROM/strength ex’s
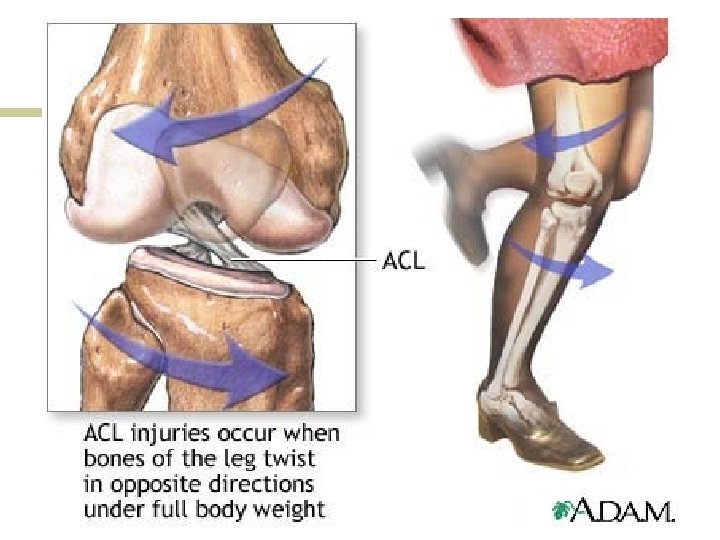
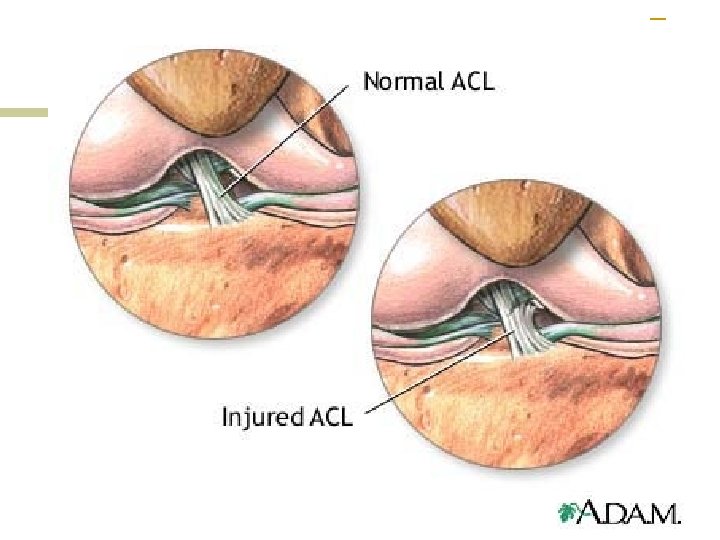
ACL anatomy
Tests of ACL At 90° Flexion + is increased translation or soft end point At 20 -30 ° Flexion (more sensitive)
Pivot Shift: ACL Injury 1. Knee extended 4. Flex Knee 2. Internally rotate tibia 5. At 20 -30°, if you feel a jerk at Ant/Lat proximal tibia, test + 3. Apply valgus load
Management of ACL tears n n PRICEMM ROM/strength ex’s as pain allows MRI Referral to Orthopedics ¡ ¡ Surgery once edema gone Graft options n n n Bone-patella-bone autograft Hamstring autograft Cadaver allograft
PCL Tear
PCL TESTS: Posterior Sag Quad Active Test Posterior Drawer
Management of PCL tears n n Immobilize; refer to Ortho If no associated injuries: ¡ n ROM /strength ex’s as pain allows If associated with other injuries: ¡ Surgical repair n n MCL Postero-lateral corner
Popliteus Tendonitis n n n Function: resists posterior translation of tibia Pain postero-lateral Garrick Test: pain with resisted ext rotation of leg Seen w/ downhill running Treatment: ¡ ¡ ¡ Modify running NSAID/ice Hamstring stretching Eccentric quad strength Refer for injection if not responding Popliteus
Flexibility testing n Inflexeruse ¡ Hamstring ¡ Quadriceps ¡ Ilio-tibial band (ITB) ¡ Gastro-soleus complex ¡ Patellar glide and tilt
Quadriceps flexibility
Hamstring flexibility: Popliteal Angle Goal: 0°
Gastro-soleus flexibility
ITB flexibility: Ober test • Tight ITB will remain Abducted • Pain = ITB injury
Ilio-Tibial Band Friction Syndrome
Management of ITB Friction Syndrome n n n Reduce run mileage/hills/banked surfaces NSAID/ice massage/phonopheresis ITB stretching Correct overpronation Gradual return-to-running program Referral for injection if fail above
Miscellaneous Tests n n Mc. Murray: Meniscal injury Apley Test: Meniscal vs ligament injury Bounce Home Test: meniscal injury, effusion Patellar grind test: PFS, chondromalacia
Normal Meniscus Meniscal Tear
Mc. Murray Test MEDIAL MENISCUS: n Flex knee maximally n Externally rotate tibia n Varus stress n Extend Knee LATERAL MENISCUS: • Flex knee • Internally rotate tibia • Valgus stress • Extend knee + is painful pop over Medial or Lateral Joint Line
Mc. Murray Test
Apley test Compression for Meniscal Injury Distraction for Ligamentous Injury
Full Flexion Test Pain at full flexion suggestive of posterior horn tear
Management of Meniscal Tears n n Weight-bearing as tolerated ROM/strength ex’s as pain allows MRI to confirm if recovery not prompt Indications for referral: ¡ ¡ Elite athletes Symptomatic after 3 months Locking Unable to fully extend knee