Klinische les 04 2012 Palliatieve behandelingen Curatieve behandelingen

Klinische les 04 -2012 Palliatieve behandelingen Curatieve behandelingen

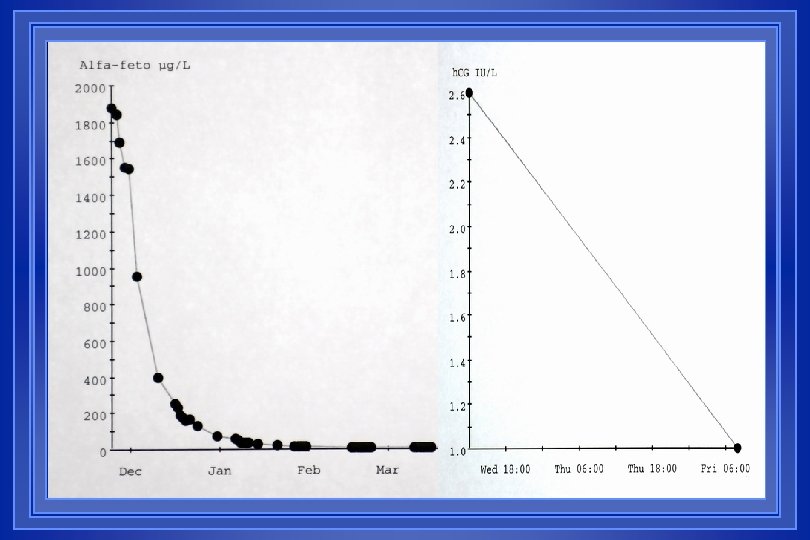
Testiscarcinoma curatie mogelijk alle stadia!!!

December 2004 VIW 890726 M 187 Gemengde kiemceltumor li testis Maart 2005 Heelkunde gepland na 4 kuren BEP Tumorafname na 2 x. BEP

Het mammacarcinoom: therapeutisch beleid volgens stadium én predictieve factoren

Het mammacarcinoom therapeutisch beleid volgens het stadium l Metastasen Hormonale behandelingen eerst indien HR+ Cytostatica upfront voor HR-; na falen HT zo HR+ Herceptin zo HER+++ (1 jaar? met of nà chemo? ) l Grote tumoren + stadia III Neoadjuvante behandelingen (HT of CT) Aangepaste lokale therapie Eventueel nog adjuvante therapie l Operabele tumoren Eerst chirurgie (z. n. gevolgd door RT) Adjuvant HT en/of CT ifv risico en receptoren Integratie taxanen en aromatase remmers l In situ hoog risico Antihormonale preventie?

Systemische therapie bij borstkanker volgens stadium en cellulaire feno-/genotype

Chemotherapie bij borstkanker - - - CMF: Cyclofosfamide, methotrexaat, 5 -FU Anthracyclines: adriamycine, epirubicine (of CAF-FEC) Liposomal doxo (Caelyx®, Myocet®) Taxanes: taxotere®, taxol® Xeloda® (Capecitabine) Navelbine® (Vinorelbine) Mitomycine ® Gemcitabine ® Herceptin® (trastuzumab) Lapatinib® Avastin®

Hormoontherapie van het borstcarcinoom

, anti-estrogens u 2000 s: - SERMs, AIs & Signal transduction inhibitors - Genomic diagnostic & predictive tests

SURVIVAL FROM DIAGNOSIS OF METASTASIS
")
Endogenous sources of sex steroids in women Ovaries Main source of estradiol (E 2) before menopause Low amounts of E 2 and testosterone (T) after menopause l Adrenals Release androstenedione (AD), direct precursor of Estrone (E 1) l Fat, muscle & tumours Contain aromatase, converting androgens into estrogens (AD --> E 1; T --> E 2) Contain 17ß OH-steroid dehydrogenase (convert E 1 into E 2) l
 Ovary androgen O O(H) HO O")
Main sites of aromatisation in women Premenopausal O(H) Ovary androgen O O(H) HO O estrogen Postmenopausal Skin Muscle Adipose Tissue Tumour

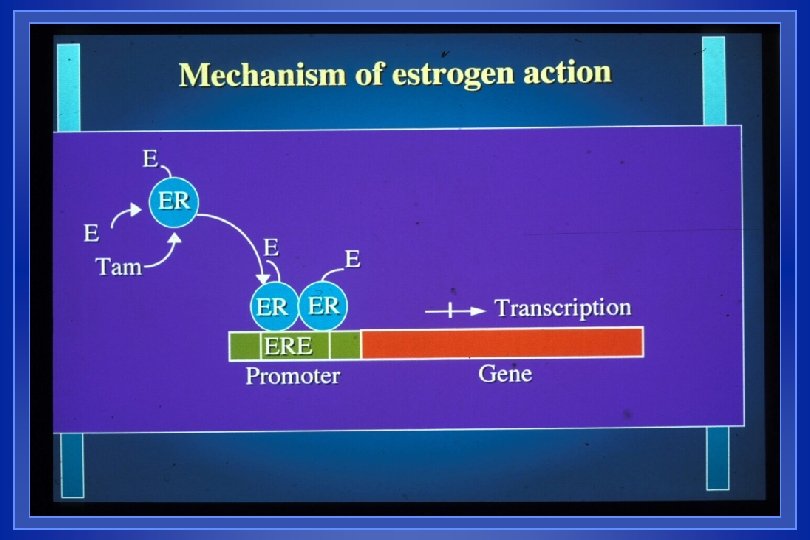
Mechanisms of Action of Hormonal Therapies l l l Block estrogen action - Tamoxifen, other anti-estrogens, (Toremifene; Faslodex) NB: dual agonistic/antagonistic action of Tamoxifen Block estrogen synthesis - Ovarian ablation (premenopausal): Surgery, RT, LHRHa (reversible) - Inhibition or inactivation of aromatase (postmenopausal): Aminoglutethimide and newer aromatase inhibitors Other mechanisms? - Progestins - Androgens - Estrogens
 and/or Tamoxifen")
Hormonal therapy: Modalities l Premenopausal women - Ovarian ablation (S, RT, LHRHa) and/or Tamoxifen (combination better) - Aromatase inhibitors + castration (mandatory) l Post menopausal women - Anti-estrogen (TAM or Analogs) - Aromatase inhibitors (steroidal <=> non steroidal) - Progestins (estrogens, androgens? ) - Optimal sequence - Withdrawal ?

Endocrine effects of Tamoxifen in preand postmenopausal women E 2 / Pg FSH /LH SHBG Ovulation Amenorrhea Ovaries Premenopause Postmenopause Increase (1 -4 x) No change Increase No change 15 -40 % Cystic changes No change Decrease Increase N. A. Decrease

HUMAN EGF RECEPTORS: HER 1, 2, 3, 4

De HER 2 receptor, prognostisch en predictief Immuunhistochemie MCA anti-HER 2 sterk + in ~25% Genetische amplificatie FISH test + in ~13%

Herceptin l Herceptin® = trastuzumab = monoclonale antistof tegen HER 2/neu (= c-erb. B 2) overexpressie bij 25% van borstkankers; genamplificatie bij 13% l Gemetastaseerde setting: enkel terugbetaald door RIZIV bij FISH+ Herceptin mono: RR 15% Herceptin + taxanes: RR 60 -80% (synergie!) l Bewezen effect in de adjuvante setting (3 -wekelijks, gedurende 1 jaar nà chemo) cfr HERA trial; liefst mèt chemo (optimale duur? ? ) l Nevenwerkingen: – allergische reactie bij 1 e toediening; – potentialisatie cardiotoxiciteit van anthracyclines
 - Pertuzumab -")
Nieuwe anti-HER 2 behandelingen MAB’s: blokkade extracellulair (+ immuun reactie? ) - Pertuzumab - TDM 1 (= trastuzumab + cytotoxisch radicaal) INIB’s: blokkade RTK intracellulair (HER 2 & andere) - Lapatinib - Neratinib
 en Stadia II hogere kans op curatie mits")
Borst. Ca Stadia I (hoog risico) en Stadia II hogere kans op curatie mits adjuvante chemo en/of hormoontherapie besluitvorming ahv prognostische en predictieve factoren

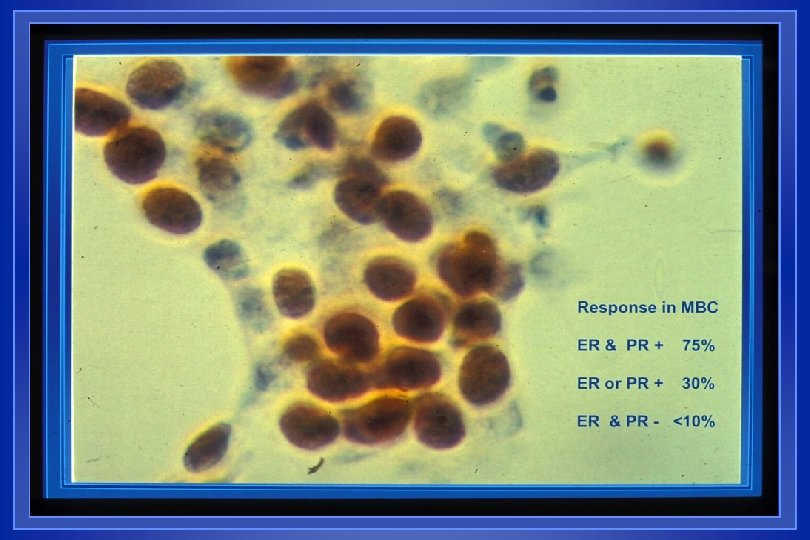
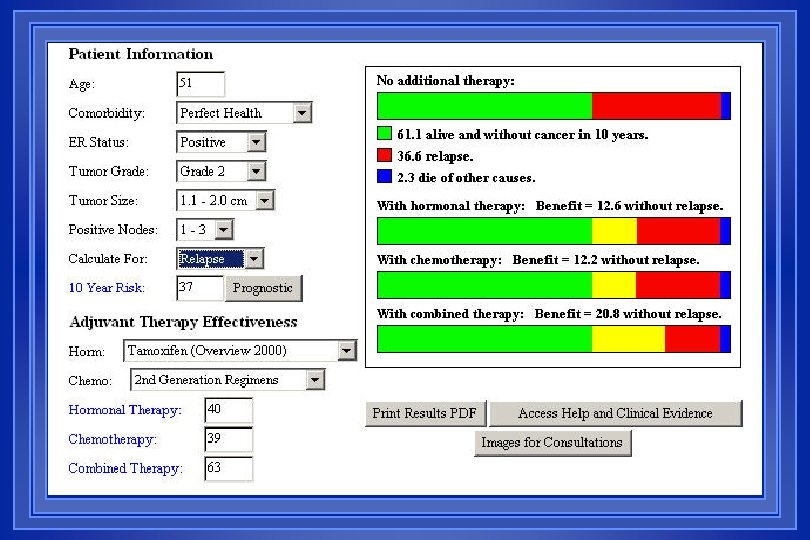
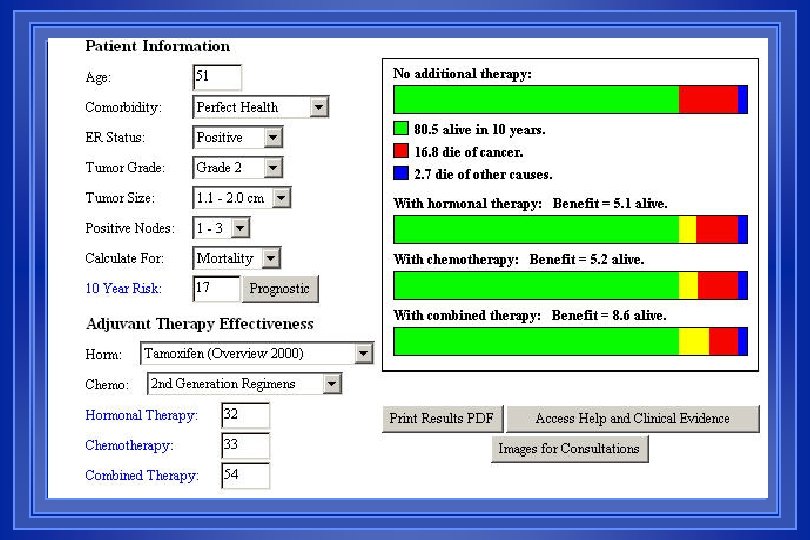
DZH 540220 V 112 – Besluitvorming adjuvante therapie 51 jaar, postmenopausaal, zelf ontdekte tumor van de linkerborst, geen macrometastasen. 08 -02 -2005: mastectomie met okseluitruiming li APO: multifocaal ILA G 2 (n=3, max 14 mm) + uitgebreid DCIS (7 cm) + LCIS Negatief snedevlak; Okseluitruiming: 1+/16, zonder KD ER en PR sterk +; c-Erb. B 2 PROGNOSE: gebaseerd op p. T, p. N, (M), differentiatiegraad (of proliferatie KI 67) én c-Erb. B 2 Stadium p. T 1 m N 1 M 0 NPI: (0. 2*1. 4 cm + 2) = 4. 28 (hoog risico, 50% herval na 10 jaar) Adjuvant on line: 10 Y recurrence 36, 6%; mortality 16, 8% PREDICTIE: respons hormoon: expressie ER & PR; geen indicatie voor Herceptin THERAPIEVOORSTEL: Adjuvante chemo (6 x FEC driewekelijks; op heden 3 x. FEC 3 x. Taxotere), waarna bestraling en hormoontherapie (Tamoxifen) 5 jaar. Adjuvant on line: relative risk reduction of recurrence is 64%, of mortality is 53%

FEC I op 22 -03 Hospitalisatie Hemokweek & kulturen Breed spectrum AB G-CSF? Nadir + febriele neutropenie op 04 -04, d 13 van FEC I

ADJUVANT TAMOXIFEN OVERVIEW OF RANDOMIZED TRIALS DURATION OF TREATMENT & EFFICACY TAMOXIFEN DURATION PROPORTIONAL REDUCTIONS IN 39, 099 PATIENTS RECURRENCE MORTALITY CONTRALATERAL B. C. 1 YEAR 18 % 10 % 13 % 2 YEARS 25 % 15 % 26 % 5 YEARS 42 % 22 % 47 % ANY DURATION 26 % 15 % 30 % ________________________________ FROM: EBCT COLLABORATIVE GROUP - LANCET (1998) 351: 1451.

Adjuvant Tamoxifen Oxford 2000 Tamoxifen 5 yrs v. Not RECURRENCES ALL DEATHS 100 80 80 68. 2% 60 54. 9% 40 40 20 20 0 5 10 15 years 64. 9% 57. 0% 60 0 5 10 15 years

Adjuvant Tamoxifen Oxford 2000 Tamoxifen 5 yrs v. Not RECURRENCES ALL DEATHS 100 Benefits 80 • 60 • • 40 • Risks 80 Improved survival 68. 2% Contralateral Ca 54. 9% Bone Cardiovascular • (Cognition) 20 • Uterine Ca 64. 9% • Thrombo-embolism 60 • (Long term agonist? ) • (HER 2+ patients? ) 40 57. 0% 20 0 5 10 15 Years

Tamoxifen efficacy & side effects
")
TAMOXIFEN VERSUS PLACEBO BMD CHANGES AFTER 12 MONTHS (mean ± SE)

ADJUVANT TAMOXIFEN OVERVIEW OF RANDOMIZED TRIALS RISK OF ENDOMETRIAL CANCER TAMOXIFEN DURATION 1 YEAR 2 YEARS 5 YEARS ANY DURATION ENDOMETRIAL CANCER INCREASE IN INCIDENCE X 2. 2 X 1. 8 X 4. 2 X 2. 6 MORTALITY 10 -YEAR RISK PER 1000 TAM CONTROL 2 1. 7 1 0 0 0. 4 FROM: EBCT COLLABORATION GROUP - LANCET, 1998; 351: 1451.

Anti-Aromatase Agents by Generation of compound • First • Second • Third Nonsteroidal Inhibitors Steroidal Inactivators Aminoglutethimide (Orimeten) Testolactone (Teslac) Fadrozole Formestane (Lentaron) Anastrozole, Letrozole (Arimidex) (Femara) Exemestane (Aromasin)

Aromatase inhibitors: side effects l Aromatase inhibitors side effects – – – l Advantages of A. I. (vs Tamoxifen) – – l Muscle pain and arthralgia Osteoporosis Effects on lipids? Letrozole , Anastrozole =, Exemestane ? Cardiac risk ? ? Gynaecological: atrophy Hot flashes No increased risk of endometrial carcinoma No increased risk of thrombo-embolism Advantages of Tamoxifen – – Decreased risk of myocardial infarction Prevention of osteoporosis

Adjuvant Trials with Aromatase Inhibitors Tamoxifen Vs. R A N D O M I Z E Anastrozole Tam + Anastrozole Letrozole Tam Exemestane ATAC 9600 pts BIG-Femta 5200 pts Letrozole MA-17 4800 pts IES 4600 pts

Adjuvante HT in Belgïe – anno 2012 l HT steeds nà CT l In situ borstca: Tamoxifen 5 jaar of nihil? Rol van AI? ikv studies (IBIS 2) Invasief borstca: - Steeds HT zo ER en/of PR aanwezig - Zo ER en PR + Tamoxifen 5 jaar ( AI 3 j ? ); meer dan 5 j? Tamoxifen 2, 5 j AI 2, 5 j; AI 5 j zo high risk - Zo ER+ en PRAI 5 jaar l
 Curatie ? R/ Neoadjuvante chemotherapie")
Lokaal gevorderd mammacarcinoom (stadium III) Curatie ? R/ Neoadjuvante chemotherapie

Lokaal gevorderd mammacarcinoom Mastitis carcinomatosa c. T 4 d
-adjuvante")
Neoadjuvante behandelingen voor grote en/of lokaal gevorderde inoperabele tumoren l Een neo (of proto)-adjuvante behandeling wordt toegediend vóór de locoregionale behandeling. l Hier is het wel mogelijk het effect op de primaire tumor te evalueren. Er wordt gehoopt dat een systemische behandeling die de meetbare tumor doet regresseren, ook een gunstig effect zal hebben op micrometa’s. l Inderdaad is de respons gecorreleerd met de prognose, vooral wanneer een pathologisch bewezen complete remissie (p. CR) wordt bereikt. l In geval van tumorregressie, kan bovendien een borstsparende behandeling worden toegepast voor o. a. borst-, larynx-, anaalkanaalen rectumkankers; ook voor osteosarcomen. Belovend voor blaas-, long-, slokdarm- en cervixcarcinomen.

Chemotherapie: neo-adjuvant Richtlijnen MBC, UZ Gasthuisberg Leuven Altijd inductie dmv systemische therapie: - Voorkeur trial. - Buiten trial 3 x. FE 100 C 3 x. Taxotere, ifv respons - Zo CI anthracyclines, voorkeur Taxotere + Cyclofosfamide (TC) of CMF tot beste respons - Zo > 69 j én sterk positieve hormoonreceptoren, R/ Tam of aromatase inhibitoren 4 à 6 m tot beste respons; zo geen respons, overweeg chemotherapie (Adria of Taxotere, eventueel wekelijks)

Chemotherapie: neo-adjuvant Richtlijnen MBC, UZ Gasthuisberg Leuven Duur chemotherapie preop ? Zo goede respons (PR, CR) of stabilisatie na 3 kuren, nog 3 kuren. l CAVE: beeldvorming correleert niet steeds met pathologische respons. l Zo progressie, stop chemo en toepassing van adequate locoregionale behandeling. l
 l Steeds")
Chemotherapie: neo-adjuvant l Respons: vooral de ’pathologische respons’ voorspelt prognose (p. CR) l Steeds gevolgd door locale therapie (meestal HK én RT) Adjuvante chemotherapie post-op? Steeds HT (>=5 j) zo HR+ l

Neoadjuvant Response to Endocrine Therapy Pre-Letrozole Miller, Lisbon, 2001 Post-Letrozole
- Slides: 45