Kingdom protista classification of protozoa phylum Protozoa Subk
 • • phylum: • Protozoa Subk. : Apicomplexa Subph:")
Kingdom protista (classification of protozoa) • • phylum: • Protozoa Subk. : Apicomplexa Subph: Ciliophora Sarcomstigophora Sarcodina Mastigophora (Amebae) (Flagellates) Parasitic Amebae Family: Endamoebidae Free-living Amebae Leptomyxidae Genus: Entamoeba Iodamoeba Endolimax Sp. gingivalis Hartmani histolytica coli dispare Microspora butschlii nana Acanthamoebidae Vahlkampfidae
 • -Prevalance rate • • - Live site - Morphology -")
Entamoeba gingivalis (non-pathogen) • -Prevalance rate • • - Live site - Morphology - cytoplasm Diagnosis: may be mistaken for E. histolytica from a pulmonary abscess
 • Prevalance: 1 to 50% • Morphology: trophozoite range 15 -50µm")
Entamoeba coli (non-pathogen) • Prevalance: 1 to 50% • Morphology: trophozoite range 15 -50µm • • ( very closely resemble E. histolytica) - cytoplasm - Pseudopodia Motility *nucleus *karyosome *peripheral chromatin
 *size: trophozoite")
Entamoeba hartmani • • • *small race of E. histolytica (morphologic similarity) *size: trophozoite < 12 mμ , c yst < 10 mμ *only clear-cut distinction between the two species is size *trophozoite ingest bacteria but no RBC

Entamoeba dispare : *There is no morphologic differences between this amoeba with E. histolytica *This amoeba no ingest RBC Iodamoeba butschlii : *Trophozoite size(4 -20μm), cytoplasm may be contain bacteria, large karyosome, small granules *Cyst size(9 -10 μm): contain glycogen vacuole, sigle nuclei

Endolimax nana • *most common of the smaller intestinal amaeba • • • *Size: trophpozoite and cyst is similar to theat of E. hartmani *Motility: sluggish pseudopodia extruded rapidly *Cytoplasm: Nucleus: contain large karyosome *Cyst:
 Family: Vahlkampfiidae Acathamoebidae Genus: Species: Naegleria fowleri Acanthamoeba")
Free-Living Amebae (Opp 0 rtuistic Amebae) Family: Vahlkampfiidae Acathamoebidae Genus: Species: Naegleria fowleri Acanthamoeba castellani calbertsoni polyphaga Leptomyxidae Balamuthia mandrillaris Habitat: in fresh, brackish and salt water, moist soil and decaying vegetation History: Human infection were first reported by Fowler in 1965 Geographic distribution: The most cases were reported from; USA, Australia, Czech, Oslovakia, Belgium, India, ……. . Epidemiology: Most cases have occurred during summer in young persons who swam or dived in swimming pools and during the ritual washing before prayer

Naegleria fowleri • Morphology , Biology and Life cycle: • • *Life cycle stage consist: -motile trophozoite: • -nonmotile cysts • *Reproduction: simple binary fission flagellate form ameboid form • *Ameboid form: found in tissue , forms a single pseudopod, • dimensions 7 by 20μm, With a nucleus contain a large central karyosome • *Flagellate form: with two flagella, pear-shaped, do not divided • *Cyst form: uninucleate, circular 7 -10μm in diameter, nucleus is similar to troph. •

Naegleria forms

Naegleria cyst & trophozoite

Life cycle
 : • Symptoms; headache,")
Symptoms and pathogeesis • Primary Amebic Meningoencephalitis(P. A. M. ) : • Symptoms; headache, fever, nausea • and vomiting accompanied by signs • of meningitis with involvement of the • olfactory, frontal, temporal, and • cerebral areas • Death : occurs early; the entire • clinical course seldom extends • beyond 3 to 6 days.
 spp. • Morhology, Biology and Life cycle: • These amebae are similar")
Acanthamoeba( Hartmanella) spp. • Morhology, Biology and Life cycle: • These amebae are similar in appearance to the ameboid stage of Naegleria but have no flagellate stage. • Cyst & Trophozoite may be found in tissue, but cysts are never seen in Naegleria infections. • Pseudopods are acanth forms

Acanthamoeba trophozoite

Free-living Amebae Life Cycle
: • *Invasion of the CNS is")
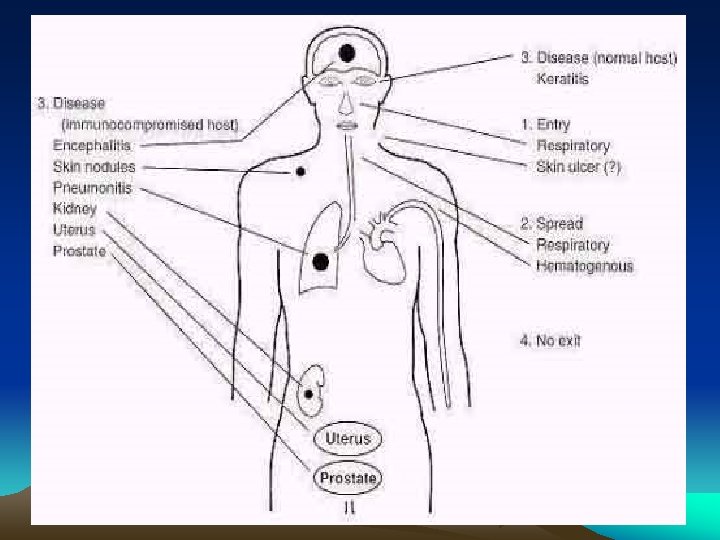
Symptoms & Pathogenesis • Granulomatous Amebic Encephalitis( GAE): • *Invasion of the CNS is not associated with swimming but is secondary to • • • infection elsewhere in the body. Amebae reach the brain by way of blood stream, likely from lung or through ulcer the skin or mucosa Occurs most often in debilitated or immunocompromised persons A. astronyxis and A. palestinensis associated only with CNS infection • Acanthamoeba Keratitis: • * Affects healthy person, increase in the number of cases in the recent • years has been linked to the wearing of contact lenses, especially soft ones. A. polyphaga and A. hatchetti only with eye infection. • Chronic granulomatous infection of the skin • A. castellani, A. culbertsoni , …. . Have causea both CNS and eye infections

Keratitis

Diagnosis of PAM and GAE: *A patient’s history of having been swimming in water 3 to 6 days prior to onset of symptoms of PAM suggest a possible diagnosis. * In brain tisse is made by microscopic identification of living or Wright-stained amebae in the patient’s CSF or trophozoites and cysts of Acanth. . * by cultivation of cerebrospinal fluid in medium non-nutrient agar seeded with living Escherichia coli for PAM and corneal scraping cultured for Acanth. Keratitis. • Treatment: At present there is no satisfactory treatment fir PAM and GAE. • *Amphotericin B, is administered intravenously in large doses; 1 to 1. 5 mģ/kg body weight daily for 3 days, followed by 1 mg/kg daily for 6 days. • *Miconazole and Rifampin are other alternative drugs.

- Slides: 21