Kidney Tumors Lecture 7 Kidney Tumors v Benign

Kidney Tumors Lecture 7

Kidney Tumors v. Benign tumors: v Most common benign tumor of kidney: v 1. Small cortical papillary adenomas. v 2. Oncocytoma. v. Malignant tumors: v. Most common malignant tumor of kidney: v. Renal cell carcinoma. v. Nephroblastoma (Wilms tumor).

Benign tumors v 1. Small cortical papillary adenomas: v. Well cirucumscibed mass, less than 0. 5 cm. v. Very common incidental findings. v. Have no clinical significance. v. Histology: Dense papillae or tubules composed of small cuboidal cells.

2. Oncocytoma v. Arises from intercalated cells of collecting ducts. v. Tumor are large in size. v. Composed of oncocytes: v. Epithelial cells with excessive amount of mitochondria, result in abundant acidophilic granular cytoplasm. v. Genetic changes: Loss of chromosomes 1, 14 & Y. v. Resample renal cell carcinomas clinically & radiologically so: v. Removed by nephrectomy to make definitive diagnosis.

Morphology: Gross: Round mass with central stellate shape scar. Histology: Cells have tan color & finely granular eosinophilic cytoplasm (large No. of mitochondria).

A characteristic appearance on X-ray: Central stellate shape scar.

Renal Cell Carcinoma: RCC v. Derived from: Tubular epithelium. v. Located predominantly in cortex. v 80 -85% of primary malignant T. of kidney. v. Most common from 6 -7 decades. v. Men are affected twice more than women. v. Higher risk in: v. Patients with polycystic disease as complication of chronic dialysis.

q. Three most common forms: 1. Clear cell carcinoma. 2. Papillary renal cell carcinoma. 3. Chromophobe renal carcinoma. 1. Clear Cell Carcinomas # Most common type: 65% of renal cell cancers. # Histologically: Cells with clear cytoplasm. # Most cases are sporadic. # May occur in familial forms. # Or in association with von Hippel-Lindau disease. (VHL).

Von Hippel-Lindau disease: v. Inherited as autosomal dominant trait. v. Cause: Mutation in tumor suppressor gene (VHL gene) on chromosomal 3 & lose of the second allele by somatic mutation. v. Loss of both copies Clear cell carcinoma. v. Characterized by predisposition to: v 1. Variety of neoplasms: A. Hemangioblastoma of cerebellum & retina. B. Bilateral multiple clear cell carcinomas. v 2. Hundreds of bilateral renal cysts.

Morphology of Clear Cell Cancers: v Solitary & large spherical masses 3 -15 cm. v. Arise anywhere in cortex. v Cut surface: Yellow to orange to gray-white. v Tumor has well defined margins.

v. Histology: Depending on amounts of lipid & glycogen inside tumor cells: v 1. Vacuolated. v 2. Solid. v. Classic vacuolated (lipid-laden), or clear cells are demarcated by their cell membranes. v. Nuclei are small & round.

v. Solid type: v. Highly anaplastic. v. Numerous mitotic figures. v. Enlarged, hyperchromatic, pleomorphic nuclei.

2. Papillary Renal Cell Carcinomas v. Show papillary growth pattern. v. Multifocal & bilateral. v. Like clear cell carcinoma: v. Occur in familial & sporadic forms. v. Unlike clear cell carcinoma: v. Not associated with abnormality of chromosome 3. Mutation: MET proto-oncogene: (Growth factor) Located on chromosomal 7. Duplications of chromosome 7 Increased dosage of MET gene Abnormal growth in proximal tubular epithelial cell Papillary carcinomas.

Morphology Gross: Necrosis, Hemorrhage, Cystic degeneration. Histology: Various degrees of papilla formation with fibrovascular cores. Cells have clear or more commonly, pink cytoplasm.

3. Chromophobe Renal Carcinomas v. Arise from intercalated cells of collecting ducts. v. Their name derives from: (Chromophobe) v. Tumor cells stain more darkly than cells in clear cell carcinomas. (They are less clear) v. Have multiple losses of entire chromosomes: v 1, 2, 6, 10, 13, 17 & 21. v. Thus, they show extreme hypodiploidy. v. Have a good prognosis.

Morphology v. Gross: Tan-brown mass. v. Histology: v Clear, flocculent cytoplasm. v. Very prominent distinct cell membranes. v. Nuclei are surrounded by halos of clear cytoplasm

Clinical Course of RCCs v. RCCs have several clinical characteristics creating difficult in diagnosis. v. Signs & symptoms vary: v. Most frequent manifestation: v 1. Hematuria: In more than 50% of cases. v. Macroscopic hematuria is intermittent & last for very short time. v. Microscopic hematuria is continuous or perminant v 2. When tumor grows largely: v. Flank pain. v. Palpable mass.

v 3. Extra-renal manifesttions: 1. Fever. 2. Polycythemia: Results from elaboration of erythropoietin by cancer cells. v 4. Paraneoplastic syndromes: v. Produce hormone-like substances resulting in: v. Hypercalcemia: Parathyroid hormone. v. Hypertension: Aldosterone hormone. v. Cushing syndrome: Hypercortisolism. v. Feminization: Estrogen. v. Masculinization: Androgen. v. In general, RCC manifests by Triad of: v 1. Painless hematuria. v 2. Palpable abdominal mass. v 3. Characteristic dull flank pain.

Wilms Tumor: Nephroblastoma v. Most common cancer in children younger than 10 years of age. v. Mostly between 2 & 5 years of age. v. Infrequent in adults. v. Contain variety of cell & tissue components, all derived from mesoderm. v. May arise sporadically or familial. v. Inherited as autosomal dominant trait.

Increased risk of development of Wilms tumor occurs in three congenital malformations: v 1. WAGR syndrome: v. Wilms tumor. v. Aniridia: Absence of iris: Colored part of eye. v. Genital abnormalities. v. Mental retardation. v 2. Denys-Drash syndrome (DDS): v. Wilms tumor. v. Gonadal dysgenesis: Abnormal organ development during embryonic growth & development. v. Renal abnormalities.

v. Genetic mutation in Both syndroms: v. Mutation of Wilms tumor 1 gene (WT 1) located on chromosome 11. v. WAGR syndrome: v. Loss of genetic material (deletions) of WT 1. v. DDS: v. Negative inactivating mutation in region of the gene, interferes with function of the remaining allele. v WT 1 gene: v. Important in normal renal & gonadal developmen v. Inactivation of one copy of this gene results in genitourinary abnormalities.
: 1. Wilms tumor. 2. Enlargement of: v. Individual body organs")
3. Beckwith-Wiedemann syndrome (BWS): 1. Wilms tumor. 2. Enlargement of: v. Individual body organs (Tongue, kidneys, liver). v. Entire body segments: Hemihypertrophy. 3. Increased risk for: Hepatoblastoma, adrenocortical tumors, rhabdomyosarcomas & pancreatic tumors. v Mutation: In WT 2 gene on chromosome 11 distal to WT 1 locus, responsible for genomic imprinting (Genomic silence), so imprinting abnormalities of growth factor predispose patient with BWS to tumor

Morphology Gross: Large, solitary, well-circumscribed tan to gray mass. Occasionally: Foci of Hg, cystic degeneration, necrosi

Microscopic examination: Characterized by: Different stages of nephrogenesis. Classic triphasic combination present in all lesions: 1. Blastemal: Sheets of small blue cells. (Embryonic) 2. Stromal: Fibrocytic. Myxoid. Skeletal muscle differentiation. v. Rarely: v. Squamous, Mucinous epithelium, Smooth muscle. Adipose tissue, cartilage, osteoid & neurogenic T. 3. Epithelial cell types: Takes the form of abortive (Primative) tubules or glomeruli.

Wilms tumor: A. Tightly packed blue cells = Blastemal component. Primitive tubules = Epithelial component. B. Focal anaplasia: Cells with hyperchromatic, pleomorphic nuclei & abnormal mitoses. A. B

Triphasic adult Wilms tumor: A. Epithelial component. B. Stromal component. C. Small areas of blastema.

v 5% of tumors contain foci of anaplasia: v. Cells with large, hyperchromatic, pleomorphic N. & abnormal mitoses. v. Presence of anaplasia correlates with: v. Presence of acquired TP 53 mutation. v. Resistance to chemotherapy. v. Distribution of anaplastic cells within primary tumor: v. Focal. v. Diffuse. v. Has important implications in prognosis.

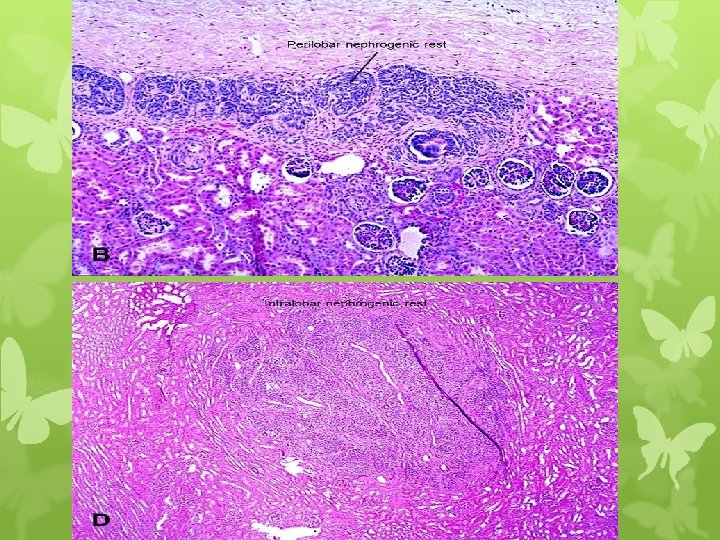
v. Nephrogenic rests: v. Embryonic T. in kidney retained after embryonic development. v. Precursor lesions of Wilms tumors. v. Sometimes present in renal parenchyma adjacent to tumor. v. Have a spectrum of histologic appearances: v. Hyperplastic rests: Masses resemble Wilms. T. v. Sclerotic rests: Consisting of fibrous tissue with immature tubules or glomeruli. v. Importance of nephrogenic rests: v. Increased risk for development of Wilms tumors in contralateral kidney.

Clinical Course v. Commonly: v. Palpable abdominal mass may extend across midline & down into pelvis. v. Less often: v. Fever. v. Abdominal pain. v. Hematuria. v. Intestinal obstruction due to pressure of tumor.

Prognosis: v. Very good. v. Excellent results are obtained with a combination of nephrectomy and chemotherapy. v. Anaplasia is associated with bad prognosis. v. Focal anaplasia that confined within the resected nephrectomy specimen: Have Good prognosis. v. Diffuse anaplasia with extra-renal spread: v. Have poor prognosis.

- Slides: 32