Kidney Transplantation Best treatment of chronic renal failure

Kidney Transplantation

Best treatment of chronic renal failure

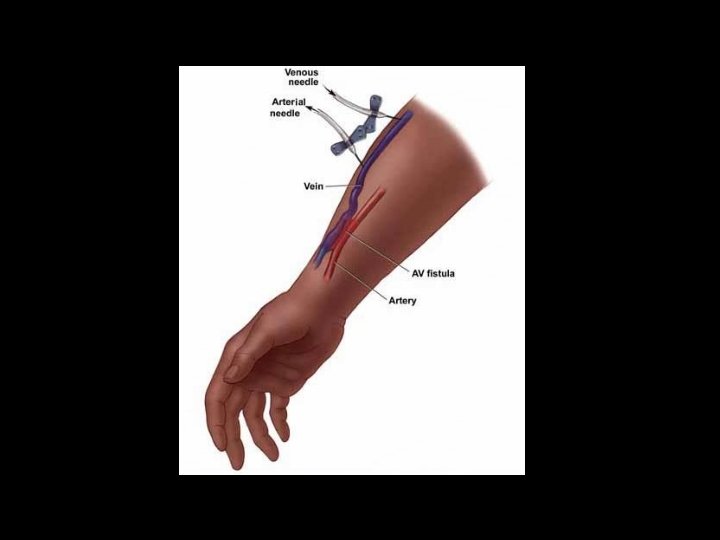
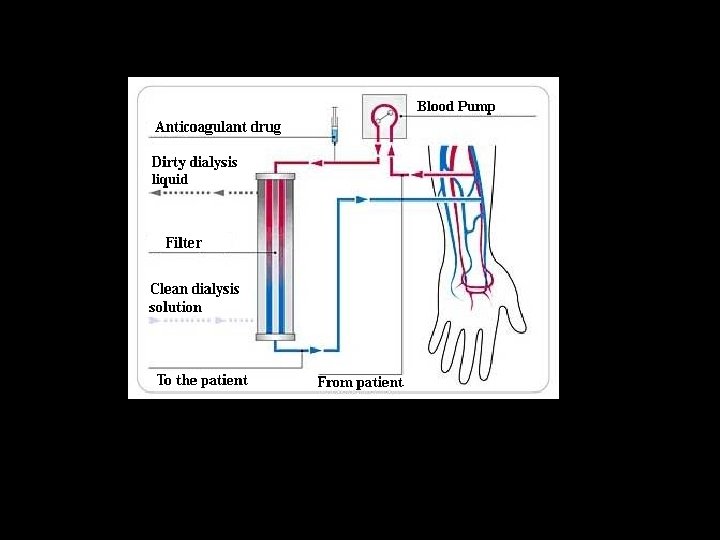
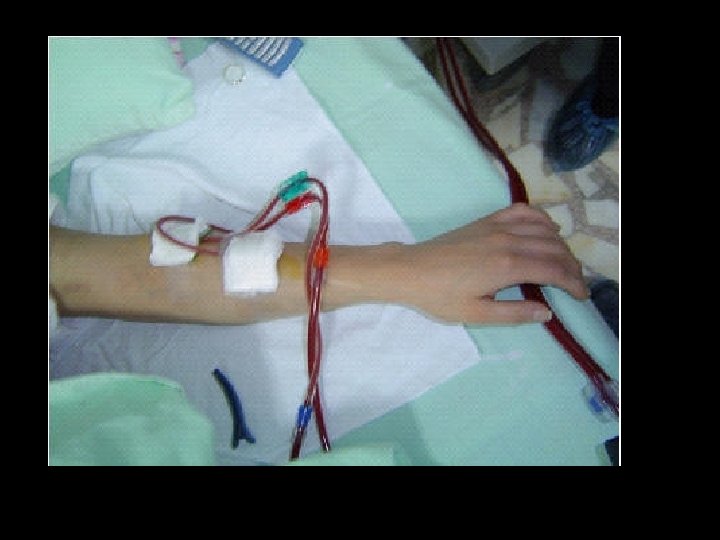
HEMODIALYSIS


PERITONEAL DIALYSIS

Renal transplantation needs donor kidney

Organ Source • Cadaver • Living donor

Yalnız kalp atacak

HLA TYPING • • • HLA ANTIGENS A B C DR LOCUS HLA A 21, A 24, B 7, B 9, DR 22
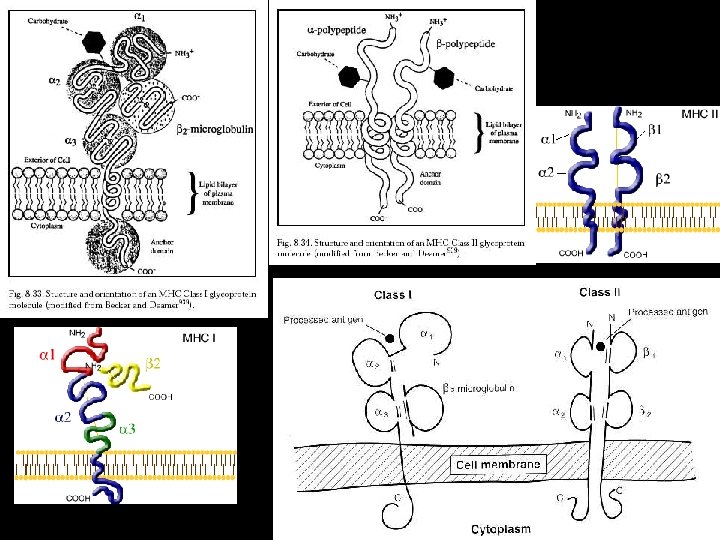
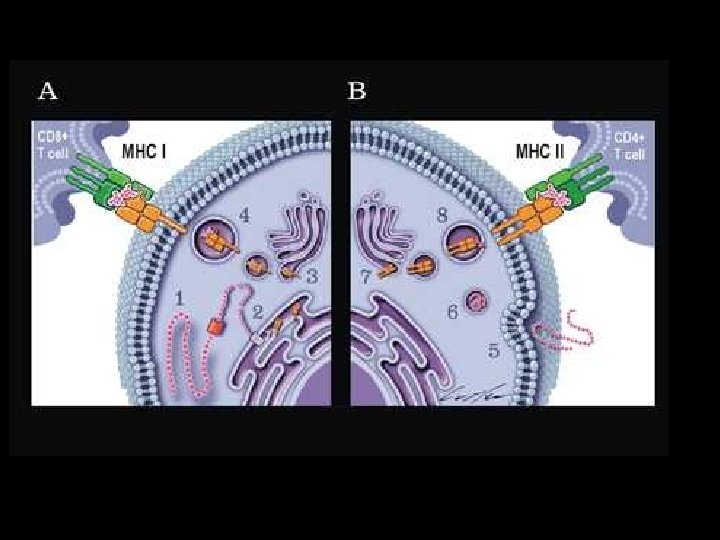

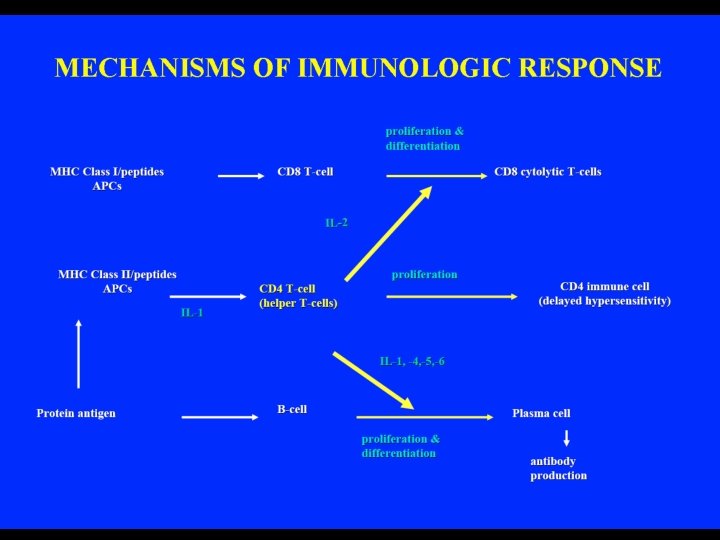
MAJOR HISTOCOMPATABILITY COMPLEX • Class I - present on almost all nucleated cells (interesting exceptions include sperm and the cells of the trophoblast). • Class II- present on Antigen Presenting Cells (macrophages, B cells, and dendritic cells). • Class III- are not surface molecules, but instead are various proteins typically which have some immunological role (C 2, C 4, Tumor necrosis factor alpha and beta, various HSPs) Human HLA region [Highly Simplified version !] ---DP--DQ--DR------C 4 --C 2 --Bf--------B--C--A--Protein Products: DPa and DPb Complement HLA-B (a) DQa and DQb TNF a & b HLA-C (a) DRa and DRb HSP proteins HLA-A (a)

Human MHC genes are highly polymorphic

HLA TYPING • • • A-MATCH…FULL B-MATCH. . ONE ANTIGEN DIFFERENT C-MATCH. . TWO ANTIGENS DIFFERENT …. . SO ON THE MORE CLOSER TO A-MATCH, THE MORE SUCCESSFULL KIDNEY TRANSPLANTATION

• RECIPIENT SHOULD NOT HAVE ANY INFECTION





IMMUNUSUPRESSION
 or cytotoxic/suppressor (CD 8+) T")
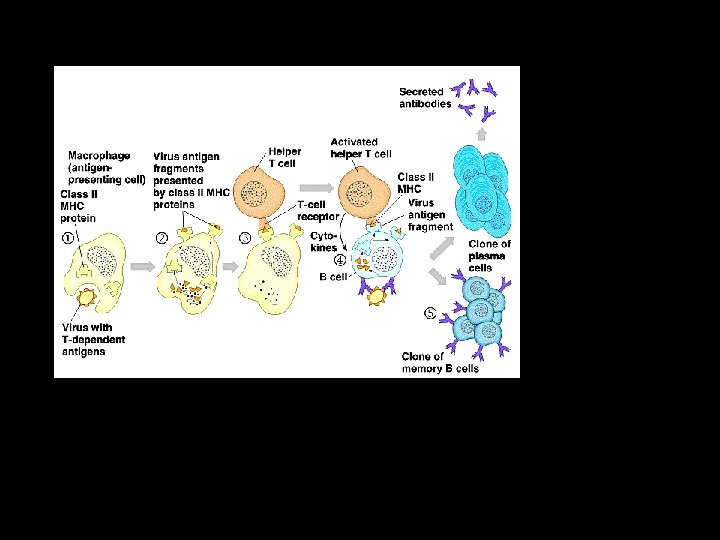
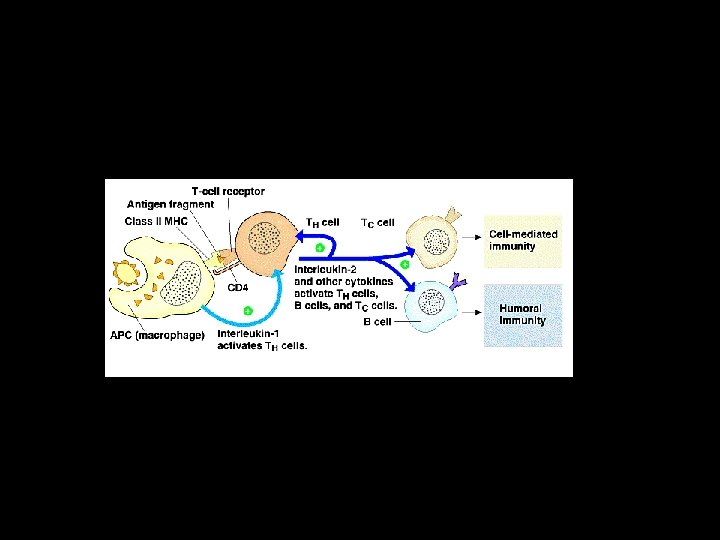
The Tc. R-CD 3 complex on helper (CD 4+) or cytotoxic/suppressor (CD 8+) T cells

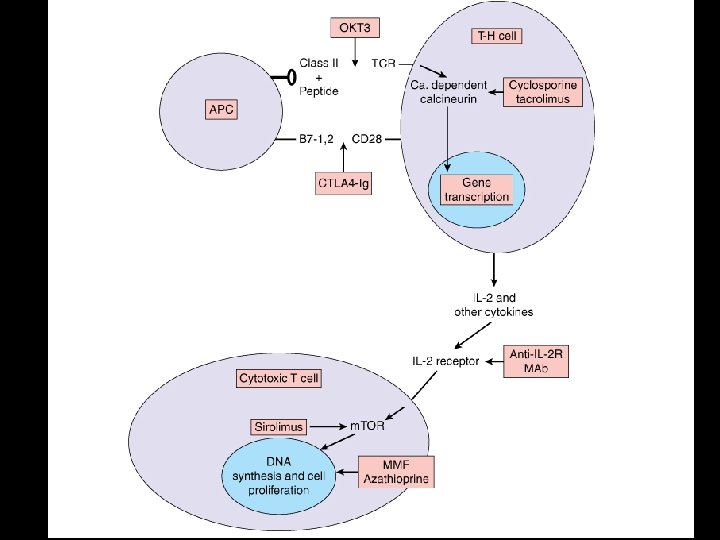
IMMUNOSUPRESSIVE AGENTS 1. T-CELL BLOCKERS 2. GLUCOCORTICOIDS 3. SITOTOXIC AGENTS 4. MONOCLONAL ANTIBODIES

T-CELL BOCKERS 1. CYCLOSPORINE-A 2. TACROLIMUS 3. SIROLIMUS CYCLOSPORINE AND TACROLIMUS ARE SELECTIVE CALCINEURIN INHIBITORS INHIBITION OF Th INDUCTION WHICH IS ACTIVATED BY IL-2

NFAT : Nuclear factor of activated T-cells FKBP: FK Binding protein
. NEUROTOXICITY (T>C). GASTROINTESTINAL PROBLEMS(T). HYPERTENSION(C>>T). HYPERKALEMIA(T).")
TOXIC EFFECTS OF TACROLIMUS AND CYCLOSPORINE. NEPHROTOXICITY (C>T). NEUROTOXICITY (T>C). GASTROINTESTINAL PROBLEMS(T). HYPERTENSION(C>>T). HYPERKALEMIA(T). HPERGLICEMIA AND DIABETES(T>C). INFECTION AND MALIGN TUMORS(BOTH)
 -Blockage of m. TOR kinase -Side Effects: -Hyperlipidemia -Anemia -Leucopenia, trombositopenia -Fever -GI")
SIROLIMUS(RAPAMYCINE) -Blockage of m. TOR kinase -Side Effects: -Hyperlipidemia -Anemia -Leucopenia, trombositopenia -Fever -GI effects, -Hypo and hyperkalemia

IMMUNOSUPRESSIVE EFFECTS OF GLUCOCORTICOIDS Inhibition of release of cytokines in T-Cells -Inhibition of antibody production in B-Cells -Inhibition of macrophages, monocytes, PMNL’s -Blockage of complement system -

SIDE EFFECS OF STEROIDS -Cushing Syndrome -Glucose intolerance -Infections -Osteoporosis -Muscle weakness
 -Azathioprine (Inhibition of")
Antineoplastic drugs as immunosupressive agents -Mycophenolat Mofetil (Inhibition of IMP dehydrogenase) -Azathioprine (Inhibition of nucleotid synthesis) -Cyclophosphamide (Alkylating agents ) -Methotrexate (Inhibitor of dihydrofolate reductase)
 (Atgam, timoglobulin) -Anti-CD 3 monoclonal antibodies (OKT 3, muromonab-CD")
BIOLOGIC IMMUNOSUPPRESSION -Antilymphosite globulines(Polyclonal antibodies) (Atgam, timoglobulin) -Anti-CD 3 monoclonal antibodies (OKT 3, muromonab-CD 3) all -mab, -imab and -umab suffixes -Anti-Tac, Anti-CD 25 monoclonal antibodies (Basiliximab, daclizumab) Anti-CD 25 Monoclonal Antibodies (Basiliximab and Daclizumab) Anti-CD 52 Monoclonal Antibody Alemtuzumab (Campath-1 h) Anti-CD 20 (Rituximab) Monoclonal Antibodies to Adhesion Molecules anti–LFA-1 m. Ab (efalizumab) anti-CD 4 m. Ab (priliximab)


PROF. DR. MEHMET A. HABERAL


16 DECEMBER 2006
 Kidney transplantation: 7 June 1997 Marriage : 2001 Baby :")
Meryem (28 years old) Kidney transplantation: 7 June 1997 Marriage : 2001 Baby : 2002

THE END
- Slides: 54