Kidney By Dr Abdel Aziz M Hussein Lecturer

Kidney By Dr. Abdel Aziz M. Hussein Lecturer of Medical Physiology

Role of ADH

Source of ADH
 Osmoreceptors: • Increase osmolarity by 1% significant increase in")
Stimulation of ADH Release 1) Osmoreceptors: • Increase osmolarity by 1% significant increase in ADH secretion. 2) Volume receptors: • Decrease blood volume by 5 -10% increase ADH secretion via the baroreceptors in right atrium, carotid sinus and aortic arch.

Role of ADH in Control of Water Output

Role of ADH in Control of Water Output 1. At thick ALH → ++ Na+, K+ & Cl- →↑ amount of solute reabs. 2. At CT and CCD → ↑ water permeability →↓ volume of H 2 O delivered to medulla from 15 ml to 5 ml → prevents irrigation of the medulla by water and loosing its high osmolarity. 3. At MCD →↑ water permeability →↑urea concentration → help urea reabsorption from PCD. 4. At PCD →↑ urea permeability → urea diffuse to the medulla increasing its osmolarity→ re-circulate between ALH and PCDs → entrapping of urea in the medulla • Urea share by 50% of osmotically active particles in medullary osmolarity especially inner medulla (600 mosmol Na. Cl and 600 mosmol urea).

Role of ADH in Control of Water Output 5. At vasa recta capillaries → ↓es medullary blood flow→ helps maintenance of medullary gradient, not dissipated (washed out) by high blood flow.

Mechanism of ADH

Mechanism of ADH

Types of Aquaporins 1. Aquaporin 1: present at the apical border of PT & DLH, not affected by ADH. 2. Aquaporin 2: present in the apical border of CD, specially principal cells. 3. Aquaporin 3: located at the basolateral border of principal cells to facilitate transport of urea & water. 4. Aquaporin 4: located in brain. 5. Aquaporin 5: located in salivary & lacrimal glands & respiratory system.

Renal Aquaporins

Diuresis and Diuretics

Diuresis and Diuretics • Diuresis means increased urine flow. • Diuretics are substances used to produce diuresis.

Water Diuresis • Done by ingestion of large amount of water. Mechanisms: 1. Water load →↓ plasma osmolarity →↓ ADH→↓ water permeability of the late DCT & CD → delivery of excess water to MCD. • Absorption of this excess water → dilute the medulla→↓ solute concentration →↓magnitude of medullary gradient 2. Water load dilutes the plasma which: a. ↑ the medullary blood flow. b. Creates ∆P for reabsorption of solutes in AVR → washout of medullary gradient.

Osmotic Diuresis • Done by ingestion of large amount of non-absorbable solute. Mechanism • Presence of non-absorbable solutes in the tubular fluid leads to: • a) ↓ Na+ & water reabsorption from PT : dilution of tubular Na+ →↓ its concentration gradient. • b) ↑ medullary blood flow → washout of the medullary gradient

Difference Between Water and Osmotic Diuresis Water diuresis Osmotic diuresis Produced by ingestion of large Produced by presence of large amount of water amount of non-absorbable solutes in tubular fluid as in: - Ingestion of mannitol. - Diabetes mellitus. Volume of urine: Volume of urine can reach larger values due to inhibition of obligatory Up to 15% of GFR 17 ml/min water reabsorption from PT Urine osmolarity: less due to Urine osmolarity: Higher than that of ↑ed free water clearance water diuresis but still hypotonic Free water clearance: wide Free water clearance: narrow Specific gravity: less Specific gravity: more Urinary Na+ concentration: is Urinary Na+ concentration: is more less

Drug Diuretics 1. Diuretics that increase GFR as caffeine. 2. Diuretics that acts by inhibition of carbonic anhydrase enzyme as diamox failure of reabsorption of Na. HCO 3 -. 3. Loop diuretics: that block co- transport of Na+- K+ - 2 Cl at thick ALH as frusemide (lasix) which is a potent diuretic. 4. Thiazide diuretics: that block Na+ - Cl- transport at the early DCT. 5. Diuretics that block Na+ channels in principle cell as amiloride or compete with aldosterone on these cells as spironolactone. Both types of diuretics prevent Na+ reabsorption in the principle cells. 6. Diuretic that block the action of ADH.

Drug Diuretics

Drug Diuretics
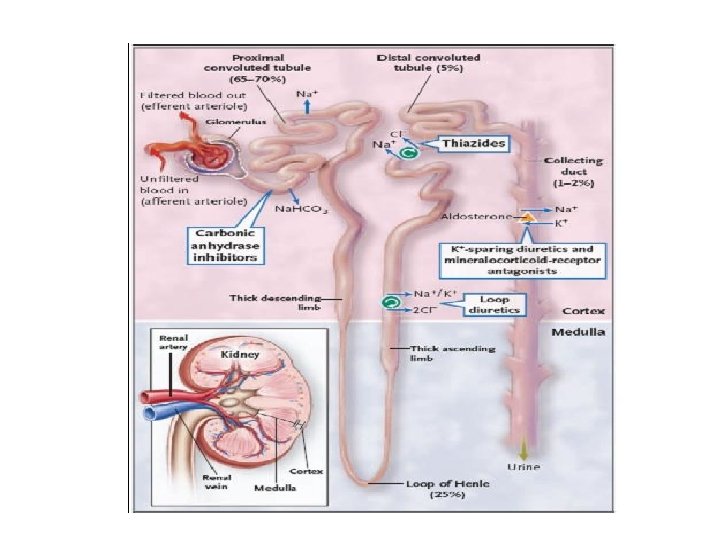

• N. B. • Of the above mentioned diuretics, amiloride and aldactone prevent K+ loss in urine so, they are called K+ -sparing diuretics while the other usually cause K+ loss in urine and so, they are called K+ - loosing diuretics.

Role of the Kidney in Acid. Base Balance

Role of the Kidney in Acid-Base Balance 1. Reabsorption of filtered HCO 3. 2. Excretion of Fixed acids with formation of new HCO 3 – Titratable acids – Ammonium ions.
 2. Thick ALH")
Reabsorption of the filtered HCO 3 1. Primarily in PT (90%) 2. Thick ALH and CDs (10%)

Mechanism of HCO 3 Reabsoption
 than water reabsorption (67%);")
• Due to more HCO 3 - reabsorption (90%) than water reabsorption (67%); HCO 3 - concentration is decreased and p. H at the end of PT is 6. 9.

Excretion of Fixed acids with formation of new HCO 3 • Fixed acids are buffered by chemical buffers mainly HCO 3 → so the pool of HCO 3 - is decreased. Example: Lactic acid + Na. HCO 3 - Na+ lactate + H 2 CO 3 CO 2 + H 2 O CO 2 is eliminated by the lung. • • • The amount of fixed acids per day 50 mmol/day So, the HCO 3 pool decrease by 50 mmol/day Thus the kidney must form new HCO 3 to replenish the lost HCO 3 by fixed acids

Excretion of Fixed acids with formation of new HCO 3 Mechanism 1. Formation of new HCO 3 with Excretion of Titratable acids 2. Formation of new HCO 3 with Excretion of Ammonium ions

A. Formation of Titratable Acids • Titratable acidity is the portion of H bound to the filtered and excreted buffers. • It equals the amount of alkali of Na. OH added to urine to bring its p. H back to 7. 4. • Or amount of H+ secreted by renal tubules and utilized for buffering of filtered alkali, other than HCO 3 -. • The filtered buffers are mainly phosphate and to some extent creatinine, urate and β-hydroxybutyrate.

A. Formation of Titratable Acids

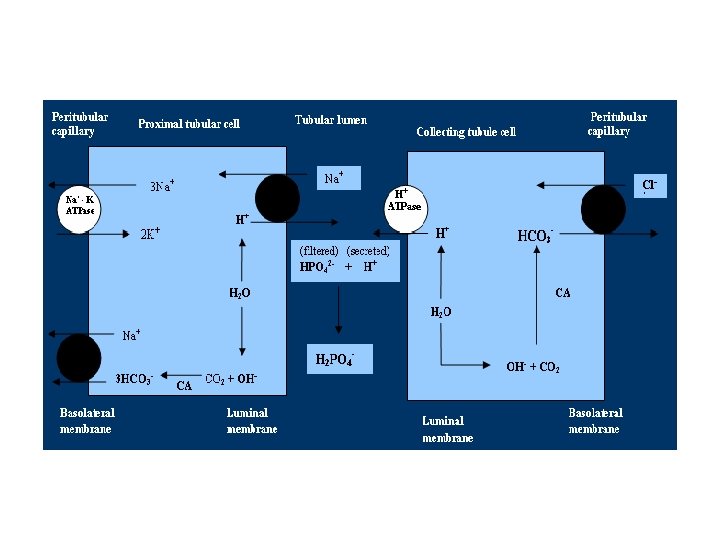
A. Formation of Titratable Acids • • In the CDs (fluid become HCO 3 free) , the secreted H combines with Na 2 HPO 4 (di-basic phosphate), to form Na. H 2 Po 4 (monobasic phosphate), the intracellular formed HCO 3 is added to the blood. For each molecule of di-basic phosphate changed into monobasic phosphate, there is formation of one molecule of HCO 3.

B. Formation of New HCO 3 and Excretion of Ammonia • NH 4 is the most important urinary buffer • It is formed in the kidney from metabolism of Glutamine

B. Formation of New HCO 3 and Excretion of Ammonia
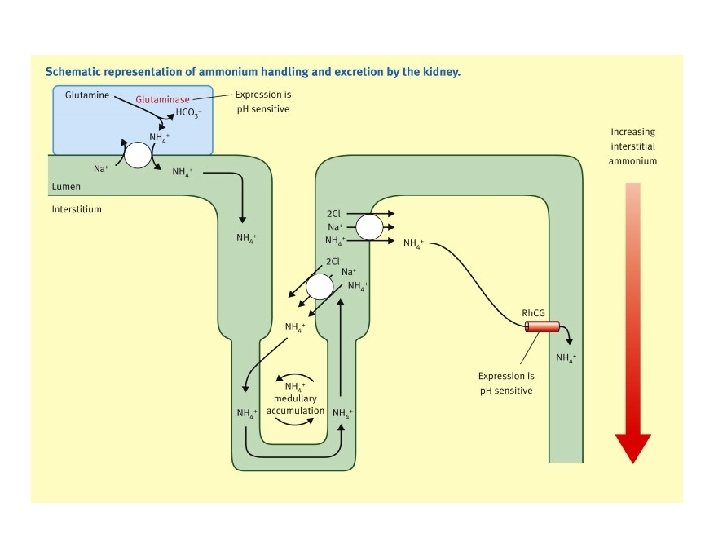

B. Formation of New HCO 3 and Excretion of Ammonia


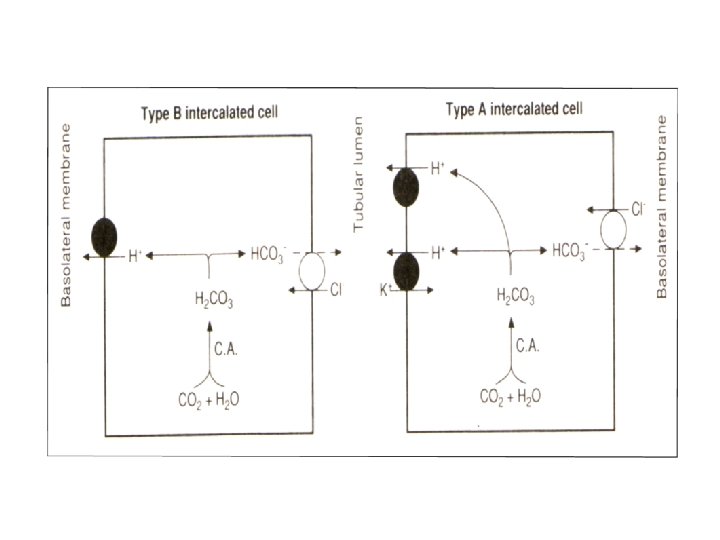
B. Formation of New HCO 3 and Excretion of Ammonia • Normally, the kidney excretes acids with NH 3 as twice as the acid excreted as titratable acidity. • In metabolic acidosis, the excretion of NH 3 can ↑ up to 500 m. Eq/day, while the excretion of titratable acidity ↑es only to 50 m. Eq/day. • In alkalosis, β intercalated cells secrete HCO 3 instead of secretion of H
 H secretion in PT and CD CDs Less amount, 75 m.")
Differences ( ) H secretion in PT and CD CDs Less amount, 75 m. Eq/day PT Greater amount about 4000 m. Eq/day Used for generation of new Used for reabsorption of HCO 3 filtered HCO 3 Secreted mainly by 1 ry Secreted mainly by 2 ry active transport by H-ATPase active mechanism in exchange or H-K ATPase with Na PH at the end of CD is 4. 6 due to p. H at the end of PCT is 6. 9 due to tight junction of the collecting leaky tight junctions ducts. Buffered by either filtered Buffered by filtered HCO 3 phosphate or mainly. ammonia Affected by aldosterone Aldosterone not affect it

Hormones and Kidney

Hormone Stimulus for Mechanism of action Effects on the kidney secretion plasma Ca 2+ Basolateral receptors Ca 2+ reabsorption in DCT. PTH adenyl cyclase c. AMP Phosphate reabsorption in PT. Stimulate 1 α hydroxylase on PT. Plasma Basolateral V 2 receptors Water permeability of the ADH c. AMP connecting tubules and CD. osmolarity. Blood phosphorylation of volume. aquaporin 2 (insertion of water channel at apical border). Ag. II. New protein synthesis by Na+ reabsorption and K+ Aldosterone Hyperkalemia. transcription. secretion by the principle cell. H+ secretion by α- intercalated cell. Atrial Stimulates guanyl cyclase GFR and decrease Na+ Atrial Naturetic pressure. enzyme c. GMP reabsorption in DT. Peptide "ANP" Angiotensin II (AII) Na+ - H+ transporter which increase H+ secretion and increase HCO 3 - reabsorption.

THANKS
- Slides: 45