KH 2220 Laura Abbott MS LMT Day 3

KH 2220 Laura Abbott, MS, LMT Day 3 Types of Joints Skull

Joints • Fibrous – Sutures of the skull, very little if any movement. • Cartilaginous – rib attachments to the sternum. Have some movement but not much • Synovial – Most moveable – all our moveable joints. • Syndesmosis – a type of fibrous joint that is a little bit moveable; found between the long bones of the body such as the radius and ulna or tibia and fibula
")
Joints l. Ball-And-Socket shoulder and hip; multiaxial l. Plane – clavicle/ scapula (AC Joint) l. Condyloid – metacarpal/phalangeal; biaxial, oval concave/convex –

Joints l. Pivot – C 1/C 2 atloaxial joint, uniaxial, rotation l. Hinge Saddle – thumb, biaxial – elbow, uniaxial, flexion/ extension

Joints • Hilton’s Law – a nerve that supplies a joint, supplies the muscles that move the joint and the skin that covers the attachments • Degenerative Joint Disease – • Osteoarthritis – • Proprioception –

Muscles • Characteristics – Excitability – the ability to – Contractility – the ability to – Extensibility – the ability to be – Elasticity – the ability to return to normal

Muscles • Functions – External mobility – Internal mobility – Produce heat – Maintain posture – Movement of lymph

Muscles • Strength – The ability of a muscle or group of muscles to • Types of muscle – Smooth: – Skeletal: – Cardiac:

Three forms of connective tissue hold the muscle cells together: • Endomysium: the connective tissue that surrounds individual muscle cells (in other words, endomysium glues adjacent muscle cells together). • Perimysium: the connective tissue that surrounds each fasciculus • Epimysium: the connective tissue that surrounds the entire muscle. The epimysium is different from the deep fascia. Whereas the epimysium wraps each skeletal muscle individually, the deep fascia is a continuous sheet that covers the entire body.
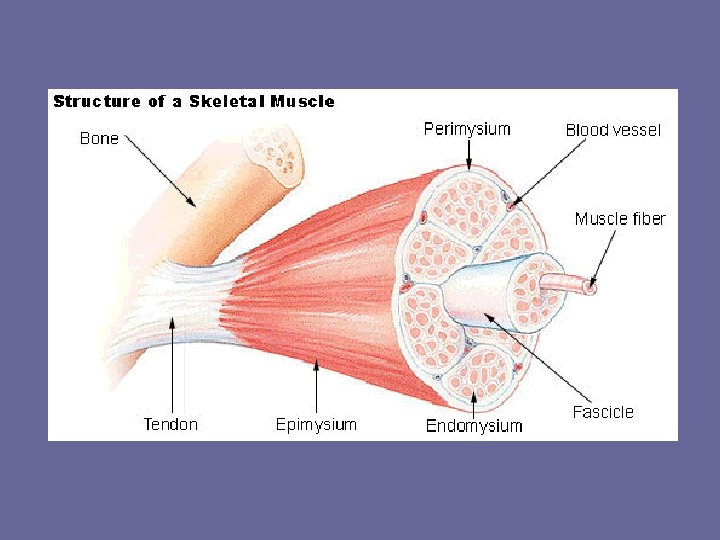

Attachment of Muscles to Bones • Skeletal muscles are attached to bone by way of tough cords of fibrous connective tissue called tendons. • In certain cases, the fibrous tissue is spread out into a broad sheet called an aponeurosis. • The tendon (or aponeurosis) fuses with the epimysium of the muscle and the periosteum (connective tissue around the bone) of the bone.

Muscles • Types of contraction – Isometric: – Isotonic • Concentric: • Eccentric:

Isotonic Contractions • Also known as dynamic contractions during these types of contractions the muscle changes length against resistance and movement occurs. – Dynamic variable – machines, cables, pulleys – Dynamic constant - free weights, body weight • This is the most common type of contraction during which the muscle can shorten or lengthen
 In this type of contraction, movement occurs as the muscle")
Isotonic Contractions: Concentric (Positive) In this type of contraction, movement occurs as the muscle is shortening. Muscles involved in concentric contractions are also known as accelerators or spurt muscles.
 In this type of contraction, movement occurs as the muscle")
Isotonic Contractions: Eccentric (Negative) In this type of contraction, movement occurs as the muscle is lengthening. For example: during the lowering phase of a biceps curl (against resistance), the biceps brachii muscle will be eccentrically contracted as you extend the elbow. The biceps brachii is contracting, but it is getting longer. Muscles involved in eccentric contractions are also known as decelerators or shunt muscles because they slow down the powerful concentric contractors.

Isometric Contractions • the muscle increases in tension by contraction but does not change its length or the angle of the joint. • Isometric contractions are important because they stabilize some joints as others are moved. • These contractions are also useful to tone muscles, which are weak from nonuse. • Although isometric exercises are great for building muscle bulk or increasing strength in certain positions, they do not increase the efficiency or endurance of skeletal muscles.

Muscle Movements • Each skeletal muscle is attached to at least two bones, which are connected by a joint. • Its 2 points of attachment are called the origin and the insertion. • When the muscle contracts (concentrically) it pulls on its 2 points of attachment so that the origin and the insertion are drawn toward each other. • In reality, one point of attachment (the origin, usually) is held firmly in place while the other point of attachment (the insertion, usually) is free to move.

Coordinating Movements • • Prime Movers or Agonists: the muscles that are primarily responsible for generating the power to produce the movement Antagonists: The muscles that oppose the prime movers. Usually lie on the opposite side of the joint and cause the opposite joint action. The antagonist allows movement to be more controlled and refined.

Coordinating Movements • Synergists: the muscles that assist the prime movers by providing extra power; changing the angle of the movement or immobilizing one part of the body so that another part has a stable base on which to maneuver. • Fixators or Stabilizers are the names given to the synergists, which provide the immobilization or stabilizing effect

Proprioceptors • Proprioceptors are sensory receptors located in muscles, tendons and joints. • They send information into the CNS about muscle length, muscle tension, and joint movements. • There are 2 proprioceptors that can be stimulated during a stretch they are muscle spindles and Golgi tendon organs.

Muscle Spindles • Found in the muscles • Prevent muscles from overstretching by creating an involuntary contraction. In other words, you get a cramp.

Golgi Tendons • Found in the tendons • Prevent muscles from over-contracting by creating an involuntary relaxation. In other words, you drop what your holding or lifting

Clinical Terms and Conditions • • • Muscle Strain: commonly called a “pull” it is an injury of a muscle or tendon due to a violent contraction, forced stretching, or synergistic failure. Most strains occur in the muscle acting as the antagonist. Strains are classified into three grades or degrees of severity: • • • First Degree involves an overstretching or a partial tear of fibers. There is typically mild pain and may be mild swelling. Second Degree occurs when the muscle or tendon is torn between 10 -50%. There is a palpable defect and joint structures cannot hold against moderate resistance. Third Degree 100% of fibers are torn and a “snap” is often heard at the time of injury. A depression in the muscle can usually be palpated and is generally painful to touch. Function is greatly altered in 3 rd degree strains.

Skull

The Skull has 5 major cavities: • • cranial cavity 2 orbits nasal cavity oral cavity

The Skull • Flat bones • Immovable joints – sutures • Frontal Bone – forehead • Zygomatic Bone – Cheekbone • Maxilla – upper jaw, bears upper teeth • Mandible – lower jaw, bears lower • Nasal Septum – bridge of nose • Nasal Bone – superior sides of nose • Temporal Bone • Parietal Bone • Sphenoid Bone – Pteriom – midpoint of H sutures -- overlies medial meningeal arteries and veins -- immediate death

Frontal Bone Sphenoid Bone Parietal Bone Temporal Bone Nasal Bone Zygomatic Nasal Septum Maxilla Mandible

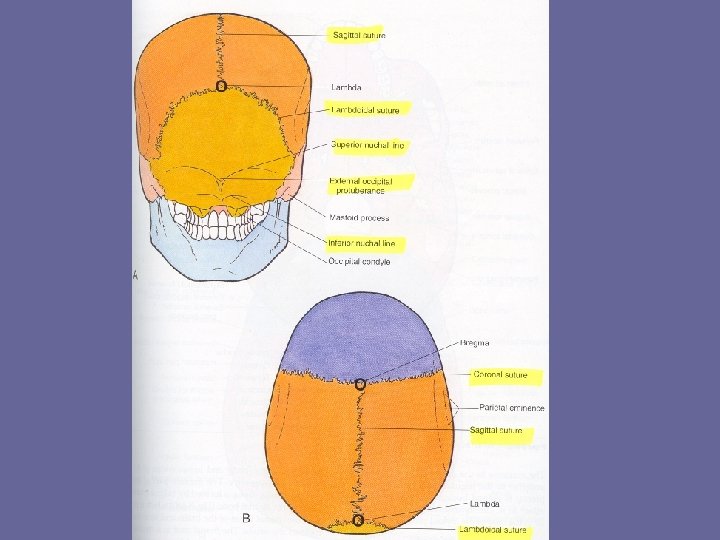
Landmarks • Posterior – External occipital protrudence – Superior and highest nuchal line • Anterior – Sagittal suture – Coronal suture – Lambdoid suture • Cranium houses brain – Above eyes and around back of ears
")
Temperomandibular Joint • Hinge joint • Temporal movements – – – Depression Occlusion (elevation) Protrusia Retrusia Lateral • Ligaments – Lateral TM ligament – Styolmandibular ligament • O: styloid process of skull
- Slides: 30