KEDARURATAN BEDAH ANAK KEDARURATAN PADA NEONATUS A Kelainan

KEDARURATAN BEDAH ANAK


KEDARURATAN PADA NEONATUS : A. Kelainan Saluran Pernafasan kongenital 1. Obstruksi jalan nafas 2. Displacement Lung volume 3. Pulmonal parenchymal insufficiency B. Kelainan Pencernaan kongenital 1. Obstruksi usus 2. Malrotasi 3. Perforrasi usus C. Defect dinding abdomen 1. Omphalocele pecah 2. Gastroschisis

Kelainan Saluran Pernafasan Kongenital A. Jenis Kelainan : 1. Saluran pernafasan bagian atas : - Mikrognatia: Pierre Robin Syndrome - Makroglosia - Choanal Atresia - Laryngeal/Tracheal stenosis - Tumor larynx dan leher

2. Kelainan Intratoraks : - Atelektasis pulmonum - Pnemotoraks - Pnemomediastinum - Kiste dan tumor paru-paru - Congenital lobar emphysema - Hernia diaphragmatika - Eventerasi diaphragma - Atresia esophagus dengan fistule trachea - Trecheo dan bronchomalacia


Operative photograph showing that upon opening the chest, a very large right upper lobe was encountered and was allowed to herniate out through the incision, thus

B. TANDA DAN GEJALA : 1. Resletlessnes 2. Tachypnea 3. Retaction 4. Cyanosis

C. DIAGNOSIS ; 1. Anamnesis : a. Riwayat kehamilan: - ibu hamil dengan hidramnion - pre eklampsia, eklampsia - selama hamil ibu pernah sakit - riwayat trauma - paritas kehamilan - penggunaan obat-obatan, alkohol, merokok

b. Riwayat kelahiran : - kesulitan melahirkan - bayi lahir melalui sectio cesaria - trauma melahirkan - penyukit pada saat melahirkan c. Gejala dan tanda awal : - tangis bayi saat lahir, sianosis, sesak nafas, - apnea, nilai APGAR yang rendah dll

2. Pemeriksaan fisik : - Inspeksi torak: simetris, asimetris dll - Gerakan pernafasan: simetris - Retraksi dinding toraks - Perkusi dinding toraks - Auskultasi : ada kelainan suara nafas dll


D. PENUNJANG DIAGNOSIS : 1. Pemeriksaan radiologis : a. Foto polos toraks b. Foto kontras saluran nafas 2. Pemeriksaan Laboratorium : a. Laboratorium rutin : DL b. Laboratorium khusus : AGD
")
ATRESIA ESOPHAGUS (panah merah)

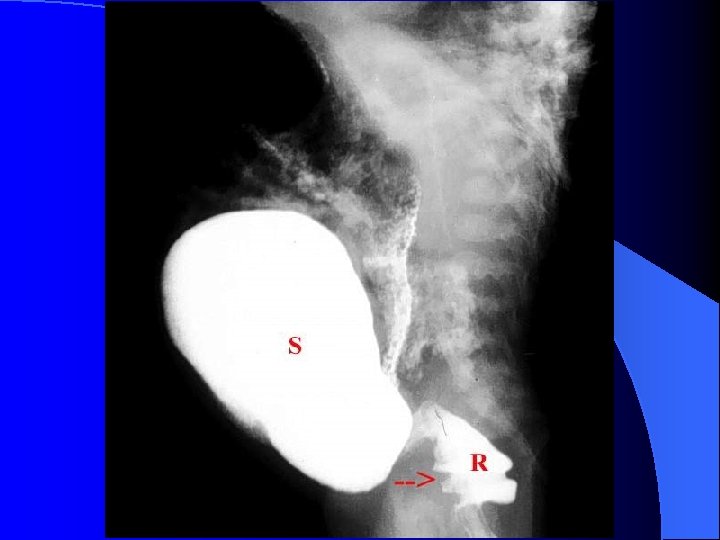
Atresia esophagus: NGT dalam segmen proksimal esophagus

Atresia Esophagus : aspirasi pnemonia

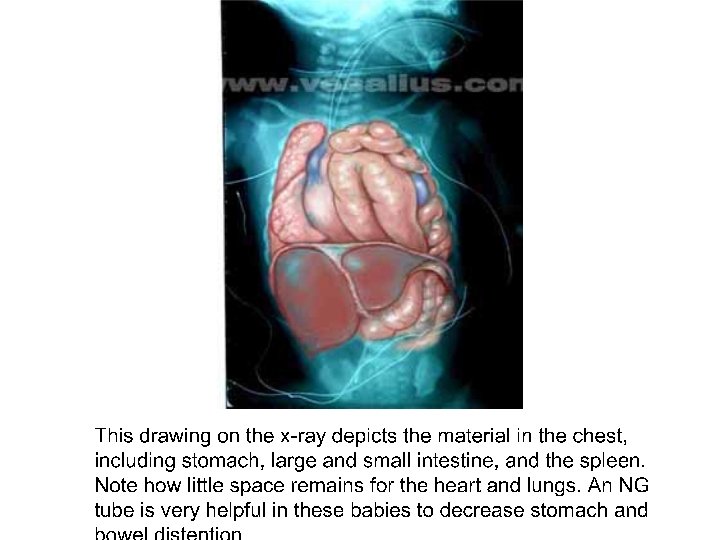
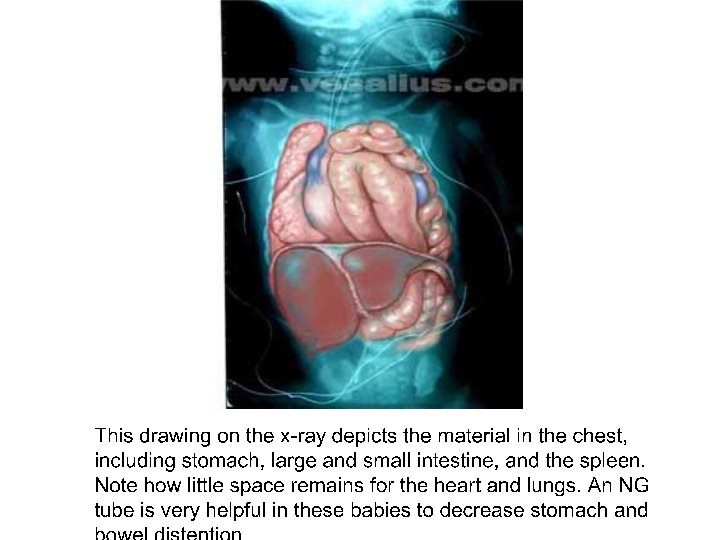
Foto polos Toraks: Hernia Difragmatika kiri

AP chest films from the day of admission demonstrate hyperinflation of the right upper lobe.

E. SIKAP DAN TINDAKAN : 1. Resusitasi jalan nafas dan pernafasan 2. Resusitasi jantung 3. Resusitasi cairan 4. Persiapan rujukan 5. Persiapan tindakan pembedahan

A clinical photograph shows the hyperexpanded right chest.

KELAINAN SALURAN PENCERNAAN KONGENITAL I. Obstruksi saluran pencernaan II. Malrotasi saluran pencernaan III. Perforasi saluran pencernaan

Skema saluran pencernaan

I. Obstruksi saluran pencernaan : A. Jenis kelainan : 1. Atresia esophagus 2. Pilorostenosis 3. Atresia duodenum 4. Atresia jejunum 5. Atresia ileum 6. Mekonium ileus 7. Mekonium plug syndrome 8. Penyakit Hirsachsprung’s 9. Anorectal malformation

 and duodenal bulb")
Operative photograph shows the massive fluid filled stomach (on the left) and duodenal bulb (on the right) which was found to contain over 400 cc of fluid.


Operative Finding : Operative photograph showing dilation of the proximal jejunum with a blind end.





B. Gejala Utama : 1. Muntah – muntah 2. Hipersalivasi 3. Distensi abdomen 4. Retensi mekonium 5. Gangguan defekasi




C. Penunjang Diagnosis : 1. Pemeriksaan radiologis : a. Foto polos abdomen b. Foto kontras saluran cerna 2. Pemeriksaan laboratorium : a. Pemeriksaan lab. rutin : Dl, UL b. Pemeriksaan Lab. Khusus
")
ATRESIA ESOPHAGUS (panah merah)

Atresia esophagus: NGT dalam segmen proksimal esophagus

Atresia Esophagus : aspirasi pnemonia

Obstruksi usus ok P. Hirschsprung’s dilatasi usus halus dan kolon tanpa udara dalam rektum

Obstruksi usus ok Intussusepsi

Obstruksi usus halus

Barium enema mekonium ileus, terlihat mikrokolon


D. Sikap dan Tindakan : 1. Bayi dipuasakan 2. Pasang pipa nasogastrik 3. Pasang infus sesuai kebutuhan 4. Berikan antibiotika sesuai indikasi 5. Letakkan bayi dalam penghangat 6. Siapkan bayi untuk dilakukan pembedahan 7. Segera rujuk bayi ke RS yang mampu menangani kasusnya


II. MALROTASI SALURAN PENCERNAAN : A. Gambaran umum : 1. Diagnosis sulit ditegakkan 2. Gejala awal tampak sebagai tanda obstruksi 3. Setiap obstruksi usus setinggi duodenum dapat dicurigai sebagai adanya malrotasi usus 4. Obstruksi usus tinggi parsial selalu disebabkan oleh malrotasi 5. Malrotasi berbahaya dan menjadi emergensi jika mengalami volvulus

Skema malrotasi usus

Skema saluran pencernaan

Malrotasi

Volvulus

Volvulus usus

Volvulus

B. PENUNJANG DIAGNOSIS : Radiologi : a. Foto polos abdomen : hilangnya gambaran udara dalam duodenum b. Foto dengan kontras enema barium : terlihat gambaran posisi sekum di daerah plexura hepatis

C. SIKAP DAN TINDAKAN : 1. Bayi dipuasakan dipasang infus 2. Pasang pipa nasogastrik 3. Berikan antibiotika sesuai indikasi 4. Persiapkan bayi untuk tindakan pembedahan 5. Segera rujuk bayi ke RS. yang mampu melakukan tindakan pembedahan

Close-up operative photograph shows the entire midgut being twisted around a single narrow mesentery.

Operative Finding : Operative photograph shows the midgut to be dusky but not necrotic.

Operative photograph showing the midgut to be dusky in color.


III. PERFORASI SALURAN CERNA : A. Gejala : 1. Distensi abdomen yang terjadi dengan cepat dan tiba-tiba 2. Bayi terlihat mengalami gangguan pernafasan 3. Liver dullnes hilang pada pemeriksaan abdomen 4. Pada perkusi abdomen tympani 5. Dengan pemeriksaan foto polos abdomen terlihat gambaran udara bebas dalam rongga peritoneum
")
B. Penyebab perforasi saluran cerna : 1. Obstruksi saluran cerna 2. Necrotizing enterocolitis (NEC) 3. Perforasi gaster spontaneus kongenital 4. Kelainan saluran nafas bagian atas kongenital C. Sikap dan tindakan : 1. Resusitasi pernafasan dan cairan 2. Pasang pipa nasogastrik 3. Berikan antibiotik sesuai indikasi 4. Funktie steril rongga peritoneum untuk dekompresi 5. Segera rujuk bayi ke RS. yang mampu untuk pembedahan
")
Necrotizing enterocolitis (NEC)

NEC Perforasi

Operative photograph shows the bowel to be white and necrotic throughout its entire length from the duodenum to the colon

Meconium ileus is most often seen in the first few days of life in neonates with cystic fibrosis, but can rarely occur in infants with a normal pancreas. In cystic fibrosis, the abnormal pancreatic secretions lead to inspissated meconium that produces intestinal obstruction. The dilated coils of ileum are opened here to reveal the inspissated green meconium (which may also be tarry or gritty), while the unopened colon at the upper left and the appendix at the lower left beyond the ileocecal valve are not dilated, and little or no meconium is passed per rectum.

Meconium peritonitis shown here as a greenish exudate overlying the serosal surfaces of the peritoneal cavity can complicate meconium ileus in utero, particularly in fetuses with cystic fibrosis. The bowel ruptures and leaks meconium, which produces a chemical peritonitis. Calcifications in the spilled meconium may be seen radiographically. Another complication of meconium ileus is volvulus.

DEFEK DINDING ABDOMEN A. Jenis kelainan : 1. Omphalocele pecah 2. Gastroschisis B. Problemnya : 1. Hipotermi 2. Hipovolume 3. Infeksi 4. Gangren saluran cerna 5. Kelainan penyerta organ lain

Omphalocele

Omphalocele
")
Omphalocele utuh (tidak pecah)

Gastroschisis

Gastroschisis

Gastroschisis

Bagian usus yang nekrosis pada gastroschisis

Pemasangan mesh pada gastroschisis

Omphalocele dengan mesh yang telah diserap

Hernia ventralis abdomen pasca repair omphalocele

Omphalocele tidak pecah dengan granulasi dan epitelisasi

")
Extrophia vesica urinaria (Exstrophia vesicae)



Extrophia Vesicae

Extrophia vesicae

C. Sikap dan tindakan : 1. Cegah pasien mengalami hipotermi dengan menempatkan bayi pada penghangat 2. Berikan infus sesuai kebutuhan untuk mencegah hipovolume 3. Antibiotika intravena sesuai indikasi untuk mencegah infeksi 4. Organ abdomen yang diluar rongga dibungkus dengan baham steril 5. Segera rujuk pasien ke RS


Kontra insisi pada kulit dinding abdomen untuk menutup defek pada gastroschisis dan omphalocele pecah

Pasca repair extrophia vesicae

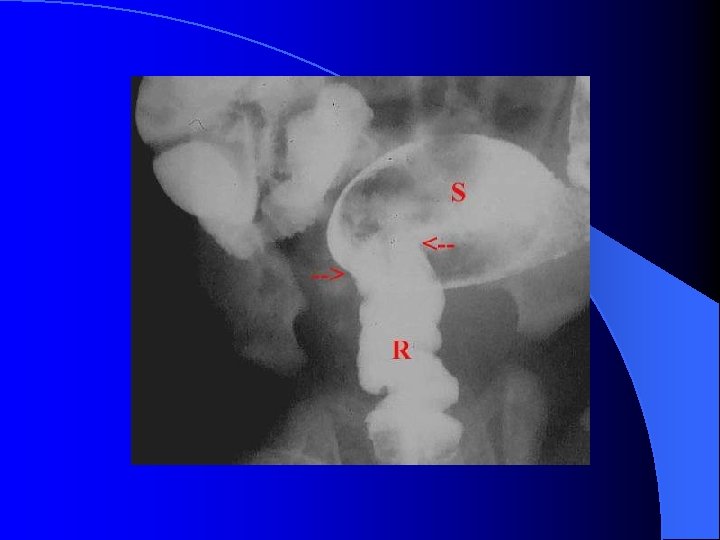
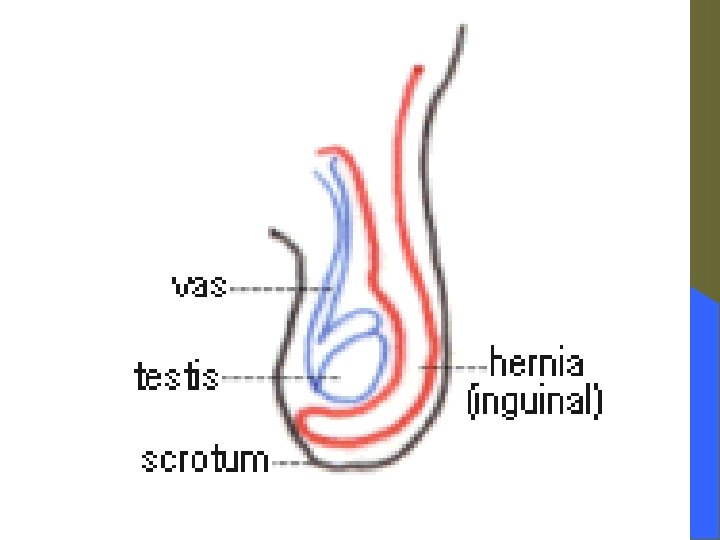
KEDARURATAN PADA ANAK-ANAK : I. Usia dibawah usia 1 tahun : 1. Hernia inguinalis strangulasi 2. Intussusepsi ( Invaginasi) 3. Obstruksi usus ok. Berbagai penyebab 4. Trauma II. Pada anak usia 1 – 6 tahun : 1. Hernia inguinalis strangulasi 2. Apendisitis akut 3. Obstruksi usus ok. Bolus askariasis 4. Trauma



A clinical photograph demonstrates the currant jelly stools.

")
Operative photograph shows the intussusception with the dusky terminal ileum (on the patient's left) protruding into the cecum (on the patient's right). Note that the appendix is intussuscepted with the ileum.

Operative photograph shows dilatation of almost the entire small bowel except for the decompressed terminal ileum in the left lower corner of the photograph.

Operative photograph is a close-up view of the area of caliber change and reveals a Meckel diverticulum with an omphalomesenteric duct remnant. This remnant had been attached to the under surface of the umbilicus, serving as a fulcrum for a small bowel volvulus.



- Slides: 105