KCMC CLUBFOOT CLINIC By Mathew Shayo MPhil CL
")
KCMC CLUBFOOT CLINIC By Mathew Shayo MPhil. CL. PT (Orthopedics and Rheumatology)

Background • • Use of Ponseti Method started back in 2008 Few staff were trained on the method Less interdisciplinary approach Students were receiving Ponseti training during their clinical rotations

Studies • Ponseti knowledge gap was established among Physiotherapists in 8 regions of Tanzania (Shayo & Van dn Bergh, 2013) • In 2014 more Ponseti knowledge gap and lack of interdiscplinarity was observed among health workers working with clubfoot children in Kilimanjaro region • Need of immediate collaboration and training

Steps • Collaboration with Usa River Rehabilitation Centre • Agreed to provide training to participants from six district hospitals in Kilimanjaro Hospital • Agreed to provide training to physiotherapist finalist students twice a year • Fellowship training to health workers • Connected our clinic to Miracle feet


Training at school of Phys

Fellowship attachment

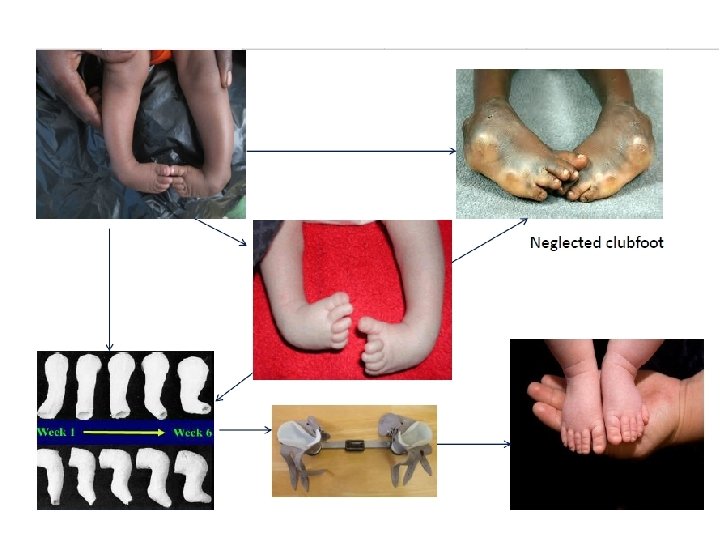
Staff are empowered to treat neglected cases

Joining Miracle feet • • • Since July 2015 Supply of material Continuous education Fellowship attachment Equipment supply Improved data collection


Statistics 1 st July - 31 st Dec 2015 Category Number of cases # of patient enrolled 25 # of patients served males females 34 25 9 Laterality: Bilateral Left Right 22 8 4 Affected relative: affected Not affected 5 25

Statistic ct. Treatment stage: Casting Tenotomy Bracing 28 1 5 Dropouts: Casting Tenotomy 7 1 Bracing: Good Fair Poor 3 1 1 # of patients with 8+ casts 3 # of visits 165 # of casting 110

Impression • Communication need to be improved • Follow-up in a near by clinics may be necessary • Parent support and education is necessary

Age of First Visit 10+yr First Visit Age 5 -10 yr First Visit Age 2 -5 yr First Visit Age 0 -3 mo First Visit Age 3 -6 mo First Visit Age 6 -12 mo First Visit Age 1 -2 yr First Visit Age 2 -5 yr First Visit Age 6 -12 mo First Visit Age 5 -10 yr First Visit Age 10+yr First Visit Age 3 -6 mo First Visit Age 0 -3 mo First Visit Age 0 2 4 6 8 10 12 14 16

Age of First Visit • Majority visits at the first three months; • there are still some cases captured at the late stage. • Community awareness may reduce/alleviate the problem in future.

Age of First Cast 12 10 8 0 -3 mo First Cast Age 3 -6 mo First Cast Age 6 -12 mo First Cast Age 6 1 -2 yr First Cast Age 2 -5 yr First Cast Age 5 -10 yr First Cast Age 4 10+yr First Cast Age 2 0 0 -3 mo First Cast 3 -6 mo First Cast 6 -12 mo First Cast 1 -2 yr First Cast Age Age 2 -5 yr First Cast 5 -10 yr First Cast 10+yr First Cast Age Age

Age of First Visit • There are still some neglected cases in the society, although few. • Further studies may be necessary. • Midwife education on early detection is necessary.

Future plans • More training to service providers in the periphery i. e. district hospitals • Regular training on advanced Ponseti • Outreach to provide early detection and referral education to midwives and traditional birth attendants. • Network with NGOs, DPOs, FBOs

Thanks Tanzania without adult disability due to clubfoot is possible
- Slides: 20