Kawasaki Disease mucocutaneous lymph node syndrome Pediatric group
 Pediatric group of Emergency department Chung-Gang Memorial Hospital")






 Acute small vessel vasculitis, pericarditis, myocarditis,")
 remittent pattern")




, especially hips, knees, or elbows ¡")




coronary aneurysms in")




- Slides: 24
Kawasaki Disease (mucocutaneous lymph node syndrome) Pediatric group of Emergency department Chung-Gang Memorial Hospital Chen, Kuan-fu M. D.
Case presentation ¡ A 3 y/o male with 5 days fever brought to ER for help again ¡ Triage: T: 39, P: 130, R: 20, BP: 120/60 ¡ Present Illness: Fever off and on Poor appearance Fair breathing Fair circulation
Case presentation ¡ Lab data CBC/DC: WBC 19 k, Hb 9. 7, MCV 87, Plt 870 k SMA: CRP 80, ESR 40, AST 120, Bil(T)3. 0 U/A: WBC 10/HPF ¡ Impression Prolonged fever, r/o UTI Abnormal liver function Skin rash
Case presentation ¡ Progress Fever still noted Shock PICU coronary aneurysm IVIG, ASA given Expired 4 days after admission
Epidemiology ¡ Incidence in TW: 66 per 100, 000 per year 2 ¡ ♂: ♀=1. 5: 1 ¡ 80% <5 y/o, most <2 y/o, rare >8 y/o ¡ <2% recurrence 3 ¡ KD is uncommon among infant<3 months In a 105755 cases of KD in Japan, 1. 67%<3 months, only 6 cases <30 days 4 U. S zero case of KD <9 weeks 5
Pathogenesis ¡ The infectious agent theory 6 1. The acute limited nature, just like toxic shock syndrome, scarlet fever 2. A seasonal peak in activity in the winter and early spring 3. The presence of both endemic and epidemic disease 4. The characteristic group 6 months~8 years
Pathogenesis ¡ The Superantigen theory 6 1. Vasculitis and arthritis 2. Infrequent person to person transmission Expansion of T-cell receptor Vβ 2+ Tlymphocytes in patients with acute KD TSST-1 secreting S. aureus, SPEB/SPEC producing group A streptococci
Pathology 6 ¡ Stage 1 (0 -9 days) Acute small vessel vasculitis, pericarditis, myocarditis, endocarditis ¡ Stage 2 (12 -25 days) Thrombotic diathesis with marked inflammation of the media of coronary arteries and other mediumsized arteries leading to formation of aneurysms. ¡ Stage 3 (28 -31 days) Regression of the acute inflammatory process. ¡ Stage 4 (40 days to 4 years) Scar formation and organization of thrombi.
Clinical Manifestations ¡ Fever ≧ 5 days, usually 7 -14 days (95%) remittent pattern with several spikes each day 7 1. Bilateral conjunctival injection (initially) 2. Oral mucous membrane changes: 1. 3. Peripheral extremity changes 1. 2. 4. 5. injected or fissured lips, injected pharynx, or strawberry tongue Acute: erythema of palms or soles or edema of hands or feet Convalescent: periungual desquamation Polymorphous rash Cervical lymphadenopathy (at least one lymph node >1. 5 cm in diameter)
1. Clinical Manifestations
Clinical Manifestations ¡ Atypical Kawasaki disease Fever and less than 4 of these 5 criteria Findings of coronary abnormalities 7 Younger, more % KD Atypical LAP 50 10 Rash 90 50 Ext. 85 60 Mucosa 90 90
Clinical Manifestations ¡ Cardiovascular: ECG changes (arrhythmias, abnormal Q waves, prolonged PR and/or QT intervals, occasionally low voltage, or ST-T wave changes); Chest x-ray abnormalities (cardiomegaly); echocardiographic changes (pericardial effusion, coronary aneurysms (20 -25%), or decreased contractility); mitral and/or aortic valvular insufficiency Aneurysms of peripheral arteries (e. g. , axillary), Angina pectoris, or myocardial infarction.
Clinical Manifestations ¡ Gastrointestinal: Diarrhea, vomiting, abdominal pain, hydrops of gallbladder, paralytic ileus, mild jaundice, and mild increase of serum transaminase levels ¡ Respiratory: Cough, rhinorrhea, and pulmonary infiltrate ¡ Neurological: Mononuclear pleocytosis in cerebrospinal fluid, striking irritability, and rarely, facial palsy
Clinical Manifestations ¡ Joint: Arthritis, arthralgia (20 -40%), especially hips, knees, or elbows ¡ Skin: Perineal rash and desquamation in subacute phase and transverse furrows of fingernails (Beau's lines) during convalescence ¡ Blood: Increased ESR, leukocytosis with left shift, positive CRP, hypoalbuminemia, and mild anemia in acute phase of illness (thrombocytosis in subacute phase) ¡ Urine: Sterile pyuria of urethral origin and occasional proteinuria
Coronary Aneurysm Commonly occur in 10 days to 4 wks ¡ Uncommonly occur >6 wks ¡ Small<5 mm, medium 5 -8 mm, giant>8 mm ¡ Factors of increased risk 7: ¡ 1. 2. 3. 4. 5. Male Age <1 y/o Signs or symptoms of carditis, including arrhythmias Fever>10 days Recurrence of fever after an afebrile period ≧ 24 hrs
Differential Diagnosis
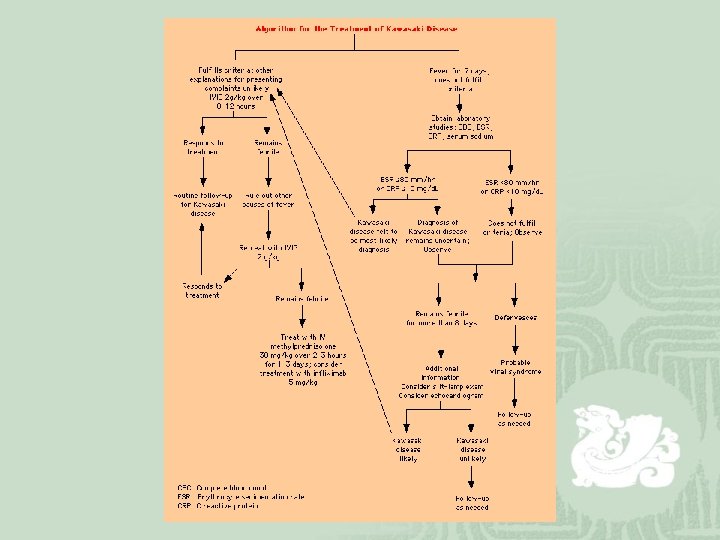
Treatment ¡ IVIG NEJM 19918: lower relative prevalence of coronary abnormalities, lower mean temperatures, a shorter mean duration of fever, indexes of acute inflammation moved more rapidly toward normal( serum albumin level, alpha 1 -antitrypsin level, and C-reactive protein level). 2 g/kg single infusion over 12 hrs within 10 days of onset of fever decrease the incidence and severity of coronary lesions (20 -25% <5%)7 Live virus vaccines (measles, mumps, rubella) should be delayed for at least 5 months after IVIG
¡ Aspirin anti-inflammatory and antithrombotic effects, 80 -100 mg/kg/d orally in 4 equally divided doses until fever subsides then 35 mg/kg qd for 6 -8 wks if no coronary arterial abnormalities 7 affected duration of fever, high-dose and lower-dose aspirin regimens have been associated with a similar incidence of coronary artery abnormalities at 30 and 60 days after disease onset. 9
¡ Steroids Controversial ¡ 1979: H Kato 10: (92 cases of KD)coronary aneurysms in 20% of cases treated with an antibiotic alone, 64. 7% of cases in the steroidtreated group, and 11% of those in the aspirintreated group ¡ 2003: Okada Y. 11: (32 cases of KD)The levels of IL-2, IL-6, IL-8, and IL-10 within 24 hours after initiating IVGG therapy were significantly lower in the G + S group than in the G group. The duration of fever was shorter, and the Creactive protein concentration decreased more quickly in the G + S group than in the G group.
Prognosis 6 ¡ ~75% resolution without sequelae ¡ ~25% coronary artery abnormalities and 55% showed regression ¡ Myocardial infarction is the principal cause of death
Reference 1. 2. 3. 4. 5. 6. Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children: clinical observation of 50 cases, Jpn J Allergol. 1967; 16: 178 -222 Chang, LY, Chang, IS, Lu, CY, et al. Epidemiologic features of Kawasaki disease in Taiwan, 1996 -2002. Pediatrics 2004; 114: e 678. Mason WH, et al, Recurrences of Kawasaki syndrome in a large urban cohort in the United States. Proceedings of the fourth international symposium on Kawasaki Disease. Dallas, Tex, AHA Tseng CF, et al, Clinical spectrum of Kawasaki disease in infants. Zhonghua Yi Xue Za Zhim 2001; 64: 168 -173 Rosenfeld EA, et al, Kawasaki disease in infants less than one year of age. J Pediatr. 1995; 126(4): 524 -529 Nasr I. et al, Kawasaki disease: an update, clinical & experimental dermatology, 26(1): 6 -12, 2001 Jan.
Adnan S et al, Diagnosis and therapy of Kawasaki disease in Children. Circulation. 1993; 87: 1776 -1780 8. Newburger JW, et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med 1991; 324: 1633 -9. 9. Durongpisitkul K, Gururaj VJ, Park JM, Martin CF. The prevention of coronary artery aneurysm in Kawasaki disease: a meta-analysis on the efficacy of aspirin and immunoglobulin treatment. Pediatrics 1995; 96: 1057 -61. 10. Kato H, Koike S, Yokoyama T. Kawasaki disease: effect of treatment on coronary artery. Pediatrics 1979; 63: 175 -9. 11. Okada Y, et al. Effect of corticosteroids in addition to intravenous gamma globulin therapy on serum cytokine levels in the acute phase of Kawasaki disease in children. Journal of Pediatrics. 143(3): 363 -7, 2003 Sep. 12. Meissner HC. Leung DY. Kawasaki syndrome: where are the answers, pediatrics. 2003 sep; 112(3 pt 1): 495 -501 7.
Thanks for Your Attention