Kawasaki Disease An Update of diagnosis and treatment




 – Febrile, irritable, toxic")
, –")


 white blood cell count 12 000/mm 3;")


 <")






. • STEROID ONLY. •")

 • IVIG: 2 g/kg as")

 until afebrile")
")

- Slides: 27
Kawasaki Disease: An Update of diagnosis and treatment
What is Kawasaki Disease? • Idiopathic multisystem disease characterized by vasculitis of small & medium blood vessels, including coronary arteries
Diagnostic Criteria • • Fever for at least 5 days At least 4 of the following 5 features: 1. Changes in the extremities § Edema, erythema, desquamation 2. Polymorphous exanthem, usually truncal 3. Conjunctival injection 4. Erythema&/or fissuring of lips and oral cavity 5. Cervical lymphadenopathy • Illness not explained by other known disease process Modified from Centers for Disease Control. Kawasaki Disease. MMWR 29: 61 -63, 1980
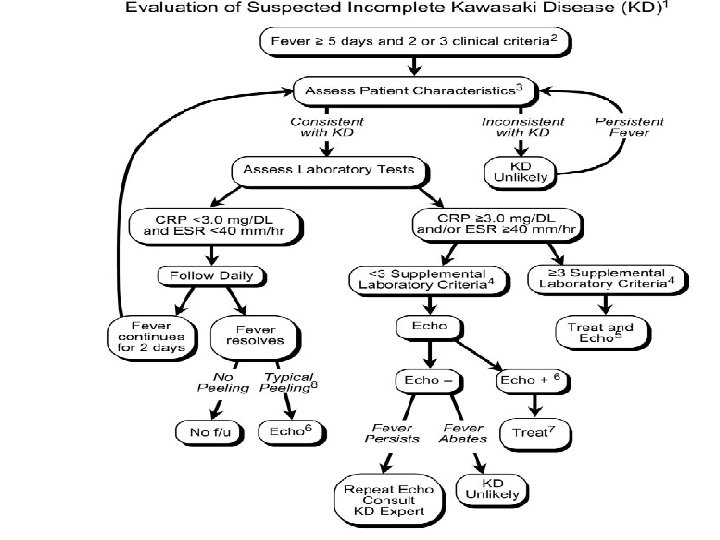
Atypical or Incomplete Kawasaki Disease • • • Present with < 4 of 5 diagnostic criteria Compatible laboratory findings Still develop coronary artery aneurysms No other explanation for the illness More common in children < 1 year of age • 2004 AHA guidelines offer new evaluation and treatment algorithm
Phases of Disease • Acute (1 -2 weeks from onset) – Febrile, irritable, toxic appearing – Oral changes, rash, edema/erythema of feet • Subacute (2 -8 weeks from onset) – Desquamation, may have persistent arthritis or arthralgias – Gradual improvement even without treatment • Convalescent (Months to years later)
• AHA classify coronary arteries aneurysms – Small (5 mm internal diameter), – medium (5 to 8 mm internal – diameter), – or giant (8 mm internal diameter). • The Japanese Ministry of Health Classify coronary arteries as abnormal • the internal lumen diameter is 3 mm in children 5 years old or 4 mm in children 5 years old; • the internal diameter of a segment measures 1. 5 times that of an adjacent segment;
Abnormal coronary artery Diameter of CA /BSA
Coronary Artery Involvement in Children With Kawasaki Disease: Risk Factors
Harada et al – risk score (1) white blood cell count 12 000/mm 3; (2) platelet count 350 000/mm 3; (3) CRP 3; (4) hematocrit 35% (5) albumin 3. 5 g/d. L; (6) age 12 months; (7) male sex. 4/7 : high risk
ASAI Symtomps 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 0 điểm Sex Nữ Age 1 Days of fever < 14 Recurrent fever Recurrent rash Recurrent bong da Anemie (Hb < 10 g/d. L) WBC(X 103/ mm 3) < 26 VS(mm) < 60 VS and PLT high for a long < 1 time(months ) Enlarge CI Abnormal rymth Ischemic myocady pericarditis 9/23 điểm : high risk 1 điểm Nam > 1 14 -15 + 26 – 30 60 – 100 2 điểm 16 + + + > 30 > 100 >1 + + +
ĐIỀU TRỊ ASPIRIN • AHA-2004: 80 -100 mg/kg. • Pediatrics-1995: meta-analysis. Control Ratio Dilated CA after 30 days (n=2547) After 60 days (n=4151) ASA 22. 8% ( 95% CI: 20. 6 -25%) 17. 1%(95% CI: 13. 6 -20. 7%) ASA+IVIG 1 g/kg 17. 3%(95% CI: 14. 3 -20. 2%) 11. 1%(95% CI: 8. 7 -13. 6%) ASA+IVIG >1 g/kg 10. 3%( 95% CI: 8. 3 -12. 3%) 4. 4% (95% CI: 2. 8 -6%) 2. 3%(95% CI: 0. 5 -4. 2%) 2. 4%(95% CI: 0. 5 -4. 2%) IVIG >1 g/kg + ASA <80 mg/kg 13%(95% CI: 9 -17%) 4. 8%(95% CI: 2. 3 -7. 4%) IVIG >1 g/kg +ASA >80 mg/kg 9. 1% (95% CI: 6. 9 -11. 4%) 4%(95% CI: 2. -6. 1%) ASA+ IVIG >1 g/kg lieàu duy nhaát
Dilated CA in 30 days Dilated CA in 60 days IVIG (2 G/KG/D) < IVIG 1 G/KG < ASA IVIG HIGH DOSE + ASA HIGH DOSE = IVIG HIGH DOSE + ASA HIGH DOSE IVIG HIGH DOSE + ASA LOW DOSE = IVIG HIGH DOSE + ASA LOW DOSE
ASPIRIN vs IVIG TỈ LỆ TỔN THƯƠNG MẠCH VÀNH IVIG+ASPIRIN -IVIG HIGH DOSE -IVIG LOW DOSE ASPIRIN
CORTICOID 1. Initial CORTICOID vs ASPIRIN. 2. Initial CORTICOID+ ASPIRIN+ IVIG vs ASPIRIN+IVIG. 3. Resistance IVIG.
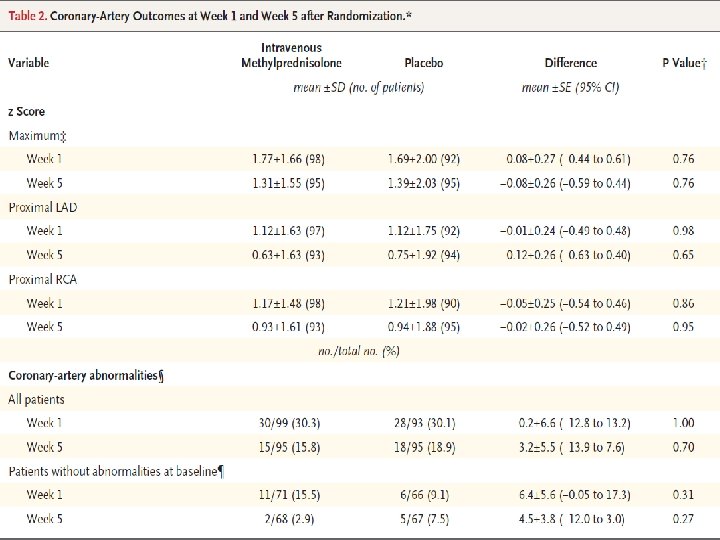
IVIG+ASPIRIN vs IVIG+ASPIRIN+ METHYPREDNISOLON Randomized Trial of Pulsed Corticosteroid Therapy for Primary Treatment of Kawasaki Disease. N Engl J Med 2007; 356: 663 -75. - 30 mg/kg over 2 to 3 hours - IVIG 2 g/kg. - Aspirin 80 -100 mg/kg.
Effect and result • Response with IVIG : 90 % • No response with IVIG : 10 %
Prediction of Intravenous Immunoglobulin Unresponsiveness in Patients With Kawasaki disease. Circulation 2006; 113; 2606 -2612; published online May 30, 2006; http: //circ. ahajournals. org/cgi/content/full/113/22/2606. Kobayashi-2006
Prediction of Intravenous Immunoglobulin Unresponsiveness in Patients With Kawasaki disease. Circulation 2006; 113; 2606 -2612; published online May 30, 2006; http: //circ. ahajournals. org/cgi/content/full/113/22/2606. TIÊN ĐÓAN TỔN THƯƠNG MẠCH VÀNH
ANTI IVIG • IVIG ONLY 2 g/kg (evidence level C). • STEROID ONLY. • PULSE STEROID + IVIG: Hashino et al + RCT. – 17 patients who did not respond to an initial infusion of 2 g/kg IVIG plus aspirin followed by an additional IVIG infusion of 1 g/kg. – Randomized to receive either a single additional dose of IVIG (1 g/kg) or pulse steroid therapy. – RESULT: • Patients in the steroidgroup had a shorter duration of fever and lower medical costs. • No significant difference in the incidence of coronary arteryaneurysms was noted between the 2 groups, but power to detect a difference was limited.
KHÁNG IVIG AHA-2004 recommends 1. Steroid treatment berestricted to children in whom 2 infusions of IVIG have been ineffective in alleviating fever and acute inflammation (evidence level C). 2. The most commonly used steroid regimen is intravenous pulse methylprednisolone, 30 mg/kg for 2 to 3 hours, administered once daily for 1 to 3 days.
Acute Kawasaki Disease: Conclusion for Treatment ( AHA 2004) • IVIG: 2 g/kg as one-time dose – Beneficial effect 1 st reported by Japanese – Mechanism of action is unclear – Significant reduction in CAA in pts treated with IVIG plus aspirin vs. aspirin alone (15 -25% 3 -5%)
Acute Kawasaki Disease: Treatment • IVIG – 70 -90% defervesce & show symptom resolution within 2 -3 days of treatment – Retreat those with failure of response to 1 st dose or recurrent symptoms Up to 2/3 respond to a second course
Acute Kawasaki Disease: Treatment • Aspirin – High dose (80 -100 mg/kg/day) until afebrile x 48 hrs &/or decrease in acute phase reactants – Need high doses in acute phase due to malabsorption of ASA – Dosage of ASA in acute phase does not seem to affect subsequent incidence of CAA
Acute Kawasaki Disease: Treatment • Aspirin – Decrease to low dose (3 -5 mg/kg/day) for 6 -8 weeks or until platelet levels normalize ( evidence level C). – No evidence /effect on CAA when used alone – Due to potential risk of Reye syndrome instruct parents about symptoms of influenza or varicella
In case of persistent or recrudescent fever: Repeat dose of IVIG 2 g/kg as single infusion; consider IV methylprednisolone 30 mg/kg once a day; may be repeated as necessary up to a total of three doses