Just an Itch Beyond Benadryl Michael Greenwald MD

Just an Itch? Beyond Benadryl™ Michael Greenwald, MD Assistant Professor, Pediatrics Emory University Children’s Healthcare of Atlanta


 and pruritis • Understand")
Objectives • Understand the relationship between pain (sensation and treatment) and pruritis • Understand basic pathophysiologic mechanisms for itching • Identify effective treatments for various causes of itching • Psychologically induce everyone here to scratch themselves at least once

#1 Help this patient • A 12 y/o with Sickle Cell Disease presents to the ED with an acute vaso-occlusive crisis. After his first dose of morphine he experiences generalized intense itching. His pain is still high (7/10). • So now you have 2 problems - what do you recommend?

#2 Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • • • Activated Charcoal Cimetidine Toradol Odansetron Diphenhydramine Topical Steroids

Part I: Understanding the Itch • • Definition Epidemiology Pathophysiology Why We Scratch
 • Inhibit mediators of")
Part II: How to treat an Itch (Understand the Cause!) • Inhibit mediators of itch • Block chemicals that induce pruritis • Treat effects of diseases which induce itching

Defining Pruritis An unpleasant localized or generalized sensation on the skin, mucus membranes or conjunctivae which the patient instinctively attempts to relieve by scratching or rubbing

Diversity of Causes and Presentation Many Causes, Many Treatments Trivial to Life threatening (mosquito bite) (malignancy) 10 -50% of cases with generalized itching have systemic disease
 • Inflammatory skin conditions (eczema, contact")
Diseases & Itching • Infections • Infestations (scabies) • Inflammatory skin conditions (eczema, contact derm, psoriasis) • Chronic Renal Failure • Cholestatic liver disease • Depression/anxiety

Assessment Challenges • No assessment tool validated to study levels of distress from itching • Most rely on 0 -10 VAS similar to pain scores

Poorly Understood & Managed • Relies on similar components of the pain system: receptors, neurotransmitters, spinal pathways and centers in the brain • Stimulating pain can relief itching • Treating pain with some analgesics relieves itching, others trigger itching • Pruritis is a common side-effect of opioid administration, sometimes worse than the pain
 • Histamine: acts")
Pruritogenic Stimuli • Pressure • Low-intensity electrical or punctate stimuli (TENS) • Histamine: acts directly on free nerve endings in skin
 Neurogenic Neuropathic Mixed Psychogenic")
Itch Pathways • • Cutaneous (pruritoceptive) Neurogenic Neuropathic Mixed Psychogenic

Pain vs Itch Nerves • Itch transmitted from specialized pain receptors: a subclass of C-nociceptors – Mechano-insensitive – Histamine sensitive • Nerve endings cluster around “itch points” which correspond to areas very sensitive to pruritogenic stimuli

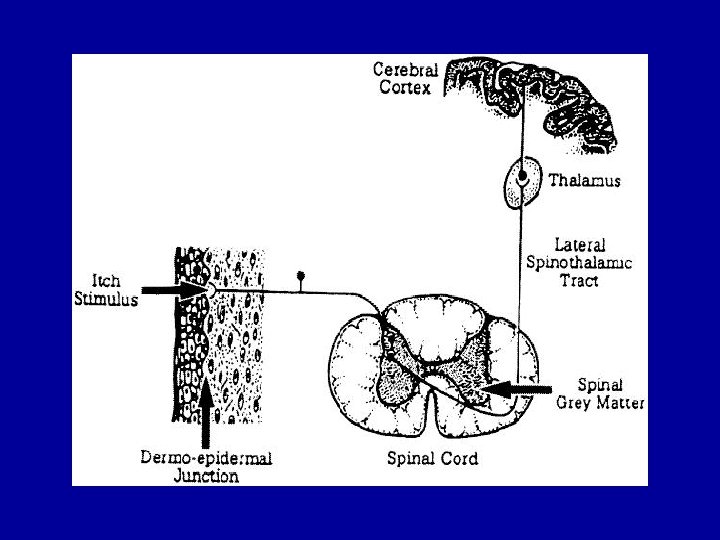
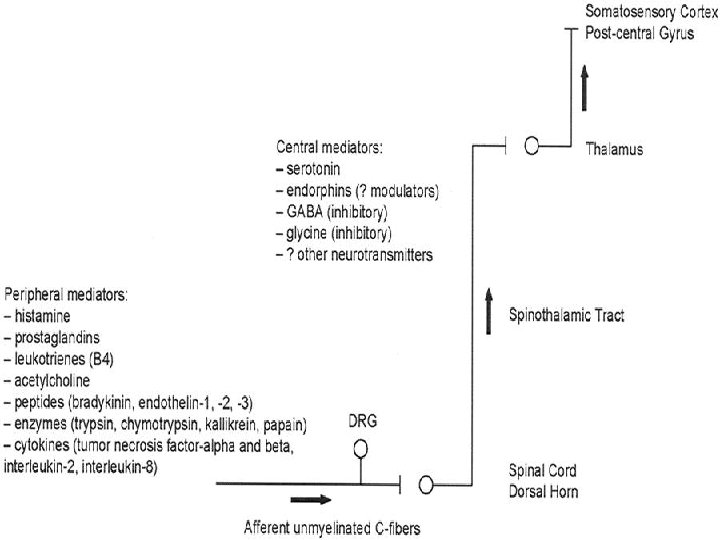
Itch pathways • • • Fibers originate @ dermal/epidermal jxn Thin unmyelinated axons, lots of branching Ipsilateral dorsal horn of spinal cord Synapse with itch-specific secondary neurons Cross to opposite anterolateral spinothalamic tract to thalamus • Somatosensory cortex of postcentral gyrus Ø SLOW transmission and BROAD receptor field

Itch Mediators • • • Histamine Prostaglandins Leukotrienes Serotonin Acetylcholine • • • Substance P Proteases Peptides Enzymes Cytokines
")
Why do you scratch? • Histamine activates both the anterior cingulate cortex (sensory, emotions) and the supplemental motor area

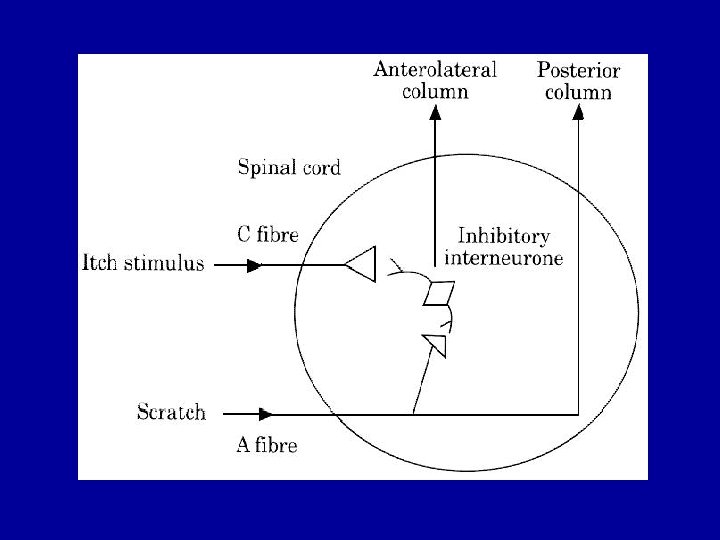
Lateral Inhibition: “Gate Theory” • Noxious stimuli of skin adjacent to pruritic trigger attenuates initial itch sensation • Scratching stimulates large fastconducting A-fibers adjacent to slow unmyelinated C fibers • A-fibers synapse with inhibitory interneurons and inhibit C-fibers
 can inhibit itching • Inhibition")
Pain & Itch • Painful stimuli (thermal, mechanical, chemical) can inhibit itching • Inhibition of pain (opioids) may enhance itching
 Ø Inhibit mediators of")
Part II: How to Treat an Itch (Understand the Cause!) Ø Inhibit mediators of itch: histamine, prostaglandins, substance P, serotonin, cytokines Ø Block chemicals that induce pruritis: opioids, antimicrobials Ø Treat effects of diseases which induce itching: eczema, CRF, LF, heme, neuro, endo

Itch Mediators: Histamine • Different effects on different H receptors • applied into epidermis itch • applied into dermis pain • Only a few types of itch relieved by anti -histamines (i. e. those caused by histamine release in the skin): insect bites, allergic skin reactions, cutaneous mastocytosis • 85% H receptors in skin are H 1 • 15% H receptors are H 2

NSAIDs for itching? • Prostaglandins cause itch directly on conjunctiva (but no effect when directly applied to skin) • Potentiates histamine elicited itch Ø Ketorolac eases itch in conjunctiva

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • • • Activated Charcoal Cimetidine Toradol Odansetron Diphenhydramine Topical Steroids

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • Activated Charcoal • Cimetidine Ø Toradol • Odansetron • Diphenhydramine • Topical Steroids
 • Neuropeptide synthesized in C-fibers @")
Substance “P” (“P” for pain and pruritis? ) • Neuropeptide synthesized in C-fibers @ DRG • Transmitted to free nerve endings to modulate pain and pruritis • Substance P containing C-fibers most abundant near junction b/epidermis & dermis (esp in lips, fingertips, prepuce and breast) • Induces pruritis directly & indirectly by releasing histamine from mast cells – Hemodialysis-associated itch – Atopic dermatitis – Psoriasis

Substance P Depletion • Capsaicin cream: excites C-fibers release substance P & calcitonin generelated peptide depletion of both –. 025% 5 times a day for notalgia paraesthetica

Other Peptides • Bradykinin: pain, inflammation & itch • Neurotension, Vasoactive Intestinal Peptide, Somatostatin, Melanocyte-stimulating hormone: histamine release from dermal mast cells

Acetylcholine • Intra-dermal injection usually burning • In eczema itching v. Independent of histamine

Serotonin • Some patients with refractory itch have been relieved by serotonin antagonist odansetron (Zofran)
")
Itch & Inflammation • Cytokines: LMW mediators of inflammatory signals b/cells (e. g. TNF) • Induce cells to secrete chemokines which cause migration of inflammatory cells from vascular space to inflammatory site
, neck, upper thorax")
Chemically induced itching: Systemic Opioids • • Usually face (trigem. nerve), neck, upper thorax 0 -90% Not necessarily related to dose incidence during pregnancy (interaction b/ estrogen & opiate receptors) • Morphine, sufentanil > fentanyl > butorphenol • Histamine is released, but not the main cause of itching • Site of injection vs distal to injection

Opioid induced itching: Systemic vs Local • Nonimmunologic release of histamine from morphine, codeine, meperidine Ø Attentuated by opioid receptor antagonists • Intradermal morphine reduced by H 1 antihistamines but not naloxone • H 2 blockers alone not effective but enhance H 1 blockers

Help this patient • A 12 y/o with Sickle Cell Disease presents to the ED with an acute vaso-occlusive crisis. After his first dose of morphine he experiences generalized intense itching. His pain is still high (7/10). • So now you have 2 problems - what do you recommend?

Help this patient • A 12 y/o with Sickle Cell Disease presents to the ED with an acute vaso-occlusive crisis. After his first dose of morphine he experiences intense itching. His pain is still high (7/10). • So now you have 2 problems - what do you recommend? Ø Nubain

Chemically induced itching: Neuroaxial • Intrathecal, epidural opioids commonly complicated by pruritis • Direct action on medullary dorsal horn and trigeminal nucleus of medulla – not t/histamine release • Blocked by naloxone (therefore opioid receptor mediated) • Also possibly related to antagonism to inhibitory neurotransmitters GABA and Glycine and 5 -HT receptors (ondansteron effective)

Chemically induced itching: Neuroaxial • Spinal anesthesia with lidocaine: 30 -100% pruritis • Fentanyl: – Intrathecal 67 -100% – Epidural 67% • Morphine – Intrathecal 62 -82% – Epidural 65 -70%

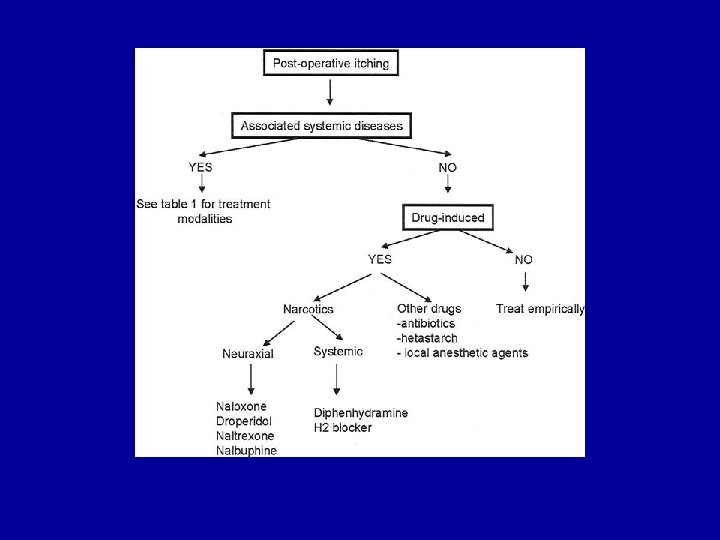
Treatments: opioid related pruritis • Diphenhydramine – for systemic opioids • For Neuraxial Opioids: – – – – Ondansteron Naloxone (1 -2 mcg/kg/hr) Nalbuphine (10 -20 mcg/kg/hr) Propofol (. 5 -1 mg/kg/hr) Lidocaine (2 mg/kg/hr) NSAIDs (diclofenac, tenoxicam) Droperidol

Chemically induced itching: Antibiotics • Penicillin: immediate type I hypersensitivity reaction • Vancomycin: massive nonimmunologic release of histamine “Red Man Syndrome” – – (flushing CP, pruritis, muscle spasms, hypotension) Related to rate of infusion Potentiated by muscle relaxants and opioids Attenuated by H 1 blockers • Rifampin

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • • • Activated Charcoal Cimetidine Toradol Odansetron Diphenhydramine Topical Steroids

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • Activated Charcoal • Cimetidine • Toradol • Odansetron Ø Diphenhydramine • Topical Steroids

Chemically induced itching: Other drugs • Fentanyl: itching decreased when mixed with bupivicane, increased when mixed with procaine • Drug induced cholestasis – esp phenothiazenes, estrogens, tolbutamide, anabolic steroids

Diseases Associated with Itching • • Renal Hepatic H Pylori Infection Hematologic d/o • • Metabolic/Endocrine Neurologic HIV Skin Diseases

Eczema & Itching • Hallmark of atopic dermatitis • >80% pts recognize stress as a trigger for increased itching • Alexithyma: Patients with chronic dermatosis who develop abnormal language development as a result of the perception that touch is noxious

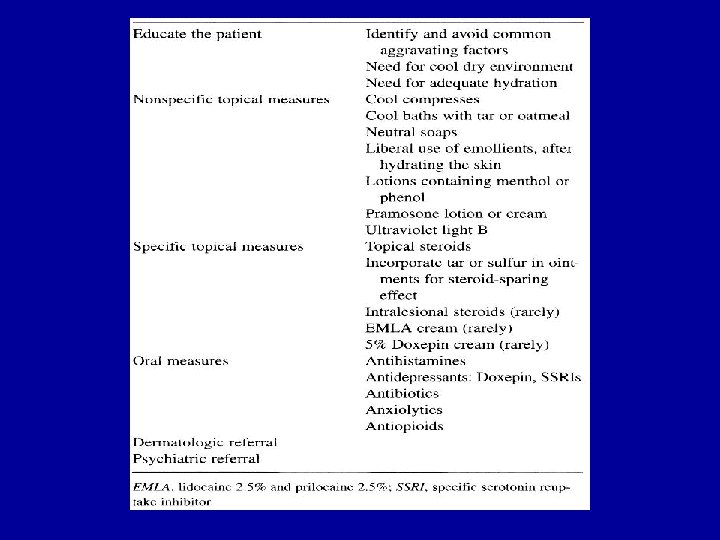
Eczema & Itching: Treatment Ø Ø Ø cool compresses emollients topical steroids antidepressants anxiolytics antibiotics

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • • • Activated Charcoal Cimetidine Toradol Odansetron Diphenhydramine Topical Steroids

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • Activated Charcoal • Cimetidine • Toradol • Odansetron • Diphenhydramine Ø Topical Steroids

Systemic Treatment: Histamine blockers • H 1 -receptor antagonists: diphenhydramine • Side effects: anticholinergic effects, paradoxical agitation, excessive sedation • H 2 -antagonists may enhance H 1 -blockers • No quality studies demonstrating efficacy of oral antihistamines for atopic dermatitis!

Renal Diseases and Itching • Chronic Renal Failure: 25 -86% itching (not in acute renal failure) • Attrib to accumulation of pruritogens: Ø histamine ( mast cells), serotonin Ø Ca, Phos, Mg, Al, vit A also implicated • 1/3 uremic patients not on dialysis • Maintenance hemodialysis: 70 -80%

Renal Diseases and Itching • Tx for uremic itching: renal transplant – Effective even when transplant is failing as long as immunosuppresants are given – Antihistamines not effective • Also effective: moisturizers, UV-B tx ( vit A in skin), oral activated charcoal, cholstyramine, naltrexone, ondansterone, topical capsaicin, azelastin, thalidomide, IV lidocaine, erythropoetin, electric needle stim

Match D/O with Antipruritic § Lymphoma § Chronic Renal Failure § Liver Failure § Conjunctivitis § Eczema § Penicillin Reaction Ø Activated Charcoal • Cimetidine • Toradol Ø Odansetron • Diphenhydramine • Topical Steroids

Hepatic Diseases & Itching • 20 -25% janudiced patients with hepatobiliary disease associated with cholestasis – 100% primary biliary cirrhosis – Viral hepatitis • Attrib to bile salts in serum and tissues • Begins palms and soles & spreads inward

Hepatic Diseases & Itching • Tx: reverse cholestatis, liver transplant • Also helpful: oral guar gum (dietary fiber) binds bile acids; cholestyramine; rifampin! (inhibits bile uptake), opioid antagonists, codeine, propofol, ondansetron • Not helpful: scratching

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • Activated Charcoal • Cimetidine • Toradol Ø Odansetron • Diphenhydramine • Topical Steroids
 hydroxyurea tx • iron def anemia,")
Hematologic Disease & Itching • Polycythemia vera (50%) hydroxyurea tx • iron def anemia, • lymphomas (Tx: cimetidine) – Hodgkins – 30% – T-cell: almost all • leukemias, plasma cell dyscrasias, mastocytosis

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • • • Activated Charcoal Cimetidine Toradol Odansetron Diphenhydramine Topical Steroids

Match D/O with Antipruritic § § § Lymphoma Chronic Renal Failure Liver Failure Conjunctivitis Eczema Penicillin Reaction • Activated Charcoal Ø Cimetidine • Toradol • Odansetron • Diphenhydramine • Topical Steroids
,")
Neurologic Disorders & Itching • Central: MS, CNS abscess, spinal and cerebral tumors (17%), CVAs – Attrib to effects on descending pathways which itching • Neurogenic – Shingles (10 -15% in US) – Notalgia paresthetica: sensory entrapment syndrome causing neuropathy of T 2 -6 dorsal spinal nerves

Endocrine D/O & Itching • • Diabetes Thyrotoxicosis Myxodema Postmenopausal syndrome Ø Most common trigger: mucocutanious candidiasis

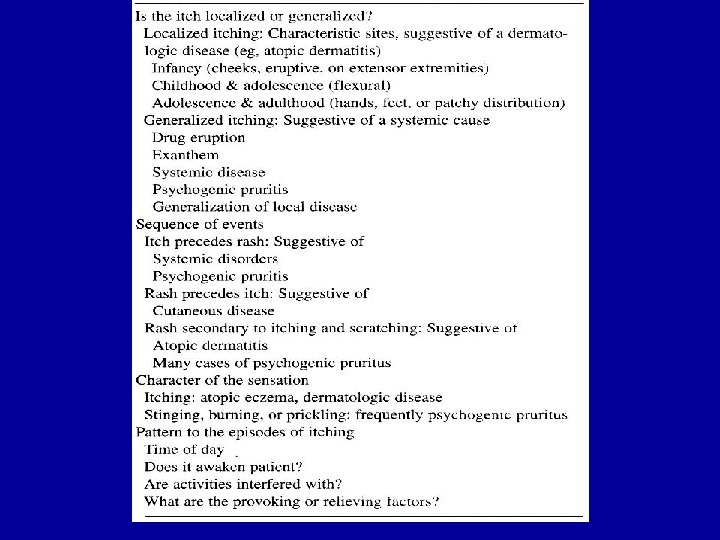
What to Ask of the Itchy Patient • • Local vs generalized? Sequence of events: itch vs rash Description of sensation Timing & severity

General Approach to Itching Ø Treat the Cause Ø Treat the Co-morbidities

Conclusions • • • Pruritis is common and often disabling Pruritis has many similarities to pain Pruritis is related but not identical to pain Effective interventions are possible Antihistamines are not always the most effective treatment

Questions?
 for biliary cirrhosis • Nalmefene (5")
Systemic Treatment: Opioids • Naloxone (. 8 mg) for biliary cirrhosis • Nalmefene (5 mg BID): – more potent and longer duration (12 -48 hrs) – May induce w/drawl sx if stopped abruptly

Take Home Points v Pain and Itching are intimately related – Cause/Triggers – Patho-physiology – Treatment v Different mechanisms for itching call for different treatments v. Antihistamines are effective for a select few causes of itching
 • Vibration, TENS for localized and")
Treatment • Cooling skin (eczema and other dermatoses) • Vibration, TENS for localized and generalized pruritis (effectiveness dissipates w/use) • UV therapy for chronic renal failure – Inhibits release of histamine and proliferation of dermal mast cells

Treatment: Topicals • Moisturizers, calamine, antihistamines, corticosteroids, EMLA • Capsaicin cream: excites C-fibers release substance P & calcitonin generelated peptide depletion of both –. 025% 5 times a day for notalgia paraesthetica
- Slides: 77