Julie Zimmerman MSN RNCOB CEFM J zimmermanrngmail com

§ Julie Zimmerman MSN, RNC-OB, C-EFM § J. zimmermanrn@gmail. com § 319 -329 -0933 § No conflicts of Interest, nothing to disclose § Opinions and Discussion by presenter

§ Identify the meaning of the Agency for Health Research and Quality’s failure to rescue and its’ impact on perinatal nursing § Review ways to improve our ability to respond to and manage the unexpected and identify consistent, reliable processes for the things we can anticipate § Identify Clinical Situations related to Intrapartum and Neonatal Care that place the patient and provider at risk

CRITICAL THINKING

§ Failure to rescue is defined as the inability of clinicians to save a hospitalized patient’s life when he or she experiences a complication (a condition not present on admission) or, more simply, the failure to diagnose and treat in time. § Failure to rescue (FTR) has been described as the end result of a series of events relating to the environment of care and nursing quality.

§ Failure to rescue occurs when a generally healthy hospitalized patient develops complications, deteriorates, and subsequently suffers an adverse outcome. The complications and deterioration likely involve subtle (and sometimes not-so-subtle) signs and symptoms that are dismissed as not being concerning or that are missed entirely. Nurses are vital to preventing failure to rescue. § There are four aspects of prevention: 1. Careful and accurate monitoring 2. Timely identification of a problem 3. Appropriate and timely intervention based on the problem 4. Activation of a team response as needed Each requires time for direct patient observation. Short-staffing decreases the ability of the nurse to spend quality time at the bedside.

§ Delay in treatment of fetal distress is the most common and costly allegation § 20% off all cases: 177 million

§ The failure to rescue rate has been suggested to be a sensitive indicator of the quality and quantity of nursing care. § Nurses are often the first members of the healthcare team to detect subtle signs and symptoms of developing complications; thus, their contribution to the rescue process is crucial. § Superb clinical assessment skills and knowledge of disease physiology are requisite to ensure early identification of complications. § Notification of other members of the team using communication styles that include clear, concise, and accurate information conveyed with appropriate urgency is also a key nursing component of a successful rescue process

§ Maternal or infant death associated with a medication error, ie § § § overdose of oxytocin, mgso 4 Death or serious disability of a fetus/infant with a normal FHR pattern on mother’s admission for labor, barring any acute unpredictable event Prolonged periods of untreated uterine tachysystole during oxytocin or misoprostol administration Ruptured uterus following prostaglandin administration for cervical ripening/labor induction to a woman with a known uterine surgical scar Infant death or disability after multiple attempts with instruments to effect an operative vaginal birth Infant death or disability after prolonged periods of coached second stage labor pushing efforts during an indeterminate/abnormal FHR pattern

Care management events: Pt death or serious injury associated with a medication error Maternal death or serious injury associated with labor or delivery in a low risk pregnancy while being cared for in a health care setting Death or serious injury of a neonate associated with labor or delivery in a low-risk pregnancy

§ Absolute avoidance of adverse outcomes is unachievable; some morbidity and mortality may not be preventable, and some degree of human error in clinical operations is inevitable. Yet improving organizational resilience and the capacity to intercept the progression of morbidity and mortality and recover from errors is within reach. Researchers have suggested that at least 50% of maternal morbidity and mortality is preventable (Geller et al. , 2004; Mitchell et al. , 2014), and several organizations and collaboratives have demonstrated that sustained implementation of multifaceted safety programs can be attained across varied settings and can improve safety attitudes, patient outcomes, or both (Grunebaum, Chervenak, & Skupski, 2011; Neily et al. , 2010; Pettker et al. , 2009; Pettker et al. , 2011; Simpson, Knox, Martin, George, & Watson, 2011; Simpson, Kortz, & Knox, 2009). Several prominent examples of successful programs are provided in Table 2.

§ Risk reduction: creating systems and supporting work environments where preventable adverse outcomes are avoided: thus reducing the possibility of litigation § Mitigation of Risk: managing liability exposure following an adverse outcome (preventable or unpreventable) § Jay Kelley

§ Jay Kelley: “ a nurse that I would like to take care of my family is frightening; I do not want to take that case to court” § Reasonableness standard is the norm with instructions to the jury § Expert testimony is used to establish standard of care, thus each side will have experts testifying to the appropriate standard of care and it will be up to the jury to ultimately decide

§ AWHONN Guidelines: Consider decreasing Pitocin when pt is greater than 5 -6 cm § Nurse’s responsibility to titrate the oxytocin based on the frequency of uterine contractions, the progress of labor and fetal tolerance. This is true no matter what induction/augmentation protocol is being used; Nurse does not get to defer responsibility § Must haves: § Knowledge of physiology of uterine contractions § Pharmacology of oxytocin § Clayworth, MCN, Vol 25, #2, March April 2000


§ Physician order on chart § Current history and physical on the chart § Prenatal record on chart § Indication for induction is documented § Pelvis is documented by physician to be clinically adequate § Estimated fetal weight within past week § Gestational age documented § Consent signed (general L&D consent) § Physician with c/s privileges is aware of induction § Status of the cervix is assessed and documented § Presentation is assessed and documented § Fetal assessment completed and indicates § A minimum of 30 minutes of monitoring § At least 2 accelerations or a bpp of 8 within the last 4 hours or moderate variability § No late decelerations in the last 30 minutes § No more than 2 variable decelerations exceeding 60 seconds and decreasing greater than 60 bpm from baseline within last 30 min

Fetal Assessment indicates: At least 1 acceleration of 15 bpm x 15 seconds in 30 minutes or adequate variability for 10 of the previous 30 minutes. No more than 1 late deceleration occurred. No more than 2 Variable decelerations exceeding 60 seconds in duration and decreasing greater than 60 bpm from the baseline within the previous 30 minutes. Uterine Contractions No more than 5 uterine contractions in 10 minutes for any 20 minute interval No two contractions greater than 120 seconds duration Uterus palpates soft between contractions If IUPC is in place, MVU** must calculate less than 300 mm Hg and the baseline resting tone must be less than 25 mm Hg. *If Oxytocin is stopped the Pre-Oxytocin Checklist will be reviewed before Oxytocin is reinitiated. ** MVU = Montevideo Units HCA Perinatal Safety Initiative Recommended Oxytocin “In Use” Checklist for Women with Term Singleton- Babies “This Oxytocin “In Use” Checklist represents a guideline for care: however, individualized medical care is directed by the physician. ” Checklist will be completed every 30 minutes. Oxytocin should be stopped or decreased if the following checklist cannot be completed. Date and time completed _______

§ Fetal status often overlooked in efforts to “get the baby out” § Physiologically inappropriate oxytocin-induced tachysystole § Supine lithotomy positioning (lumbosacral spine and lower extremity nerve injuries) § Fundal pressure (should be extinct) § Foley catheters during pushing efforts § Lack of patience/convenience over safety § Routine episiotomy § Operative vaginal Birth

§ Majority of perinatal claims occurred in the second stage, missteps in communication, delays in response in fetal distress and a timely rescue § Failures in clinical judgment fueled by loss of individual perspective (situational awareness) and lack of collaborative discussion

§ The record of both the FHR and uterine activity should be of adequate quality for visual interpretation. A full description of an EFM tracing requires a qualitative and quantitative description of: 1. Uterine contractions. 2. Baseline fetal heart rate. 3. Baseline FHR variability. 4. Presence of accelerations. 5. Periodic or episodic decelerations. 6. Changes or trends of FHR patterns over time. § The individual components of defined FHR patterns do not occur independently and generally evolve over time

Controversies Discussions Arguments

§ Maternal fetal status will be monitored during labor based on ACOG criteria for risk status (low risk women q 30 min first state, q 5 min second stage, ; high risk women q 15 min first stage, q 5 min second stage) § Indeterminate or abnormal FHR pattern will be identified within time frame for monitoring based on ACOG criteria for risk status § Appropriate intrauterine resuscitation measures based on the FHR pattern will be initiated in a timely manner § If intrauterine resuscitation measures do not resolve the indeterminate of abnormal FHR pattern, appropriate team members will be notified, come to the bedside for evaluation and if necessary, plan for expeditious birth § Michigan Keystone project, Simpson & Knox

§ In obstetric practice, disagreement regarding oxytocin use is one of the most common sources of conflict between physicians and nurses. Nurses primarily express concern over safety issues and the risks inherent in aggressive use of oxytocin, whereas many physicians express concerns related to establishing adequate labor and employing enough oxytocin to achieve delivery. These competing concerns can result in disagreement that may escalate to the point of disruptive behaviors. Lisa Miller: Oxytocin, Excessive Uterine Activity and Patient Safety, 2009

§ In spite of its widespread use, EFM is surrounded by controversy. The source of the controversy lies in its limitations. § Current study demonstrates that increased uterine activity is significantly associated with a higher incidence of an umbilical artery p. H of 7. 11 or less § Contraction monitor deserves full attention § Bakker et al, 2007 AJOG

Assess the oxygen pathway Begin corrective measures Clear the obstacles to rapid delivery Does not commit you to delivery Individual characteristics – Facility, Staff, Mother, Fetus, Labor § Delivery § Standardized approach to intrapartum FHR definition, interpretation and management demonstrates reasonableness and prudence § 2 elements that define the standard of care

§ Study of 48, 529 women at term in labor § Doubling of tachysystole with any oxytocin (dose-response correlation) § FHR changes in 25% of tachysystole events § Tachysystole increases change of composite neonatal morbidity

§ Always need 60 seconds § Identify what it is and what is not § Miller, Lisa (AWHONN national conference, 2013)

§ Culture § Communication § Team training in high risk events (shoulder dystocia, emergency c/s, hemorrhage, neonatal resuscitation) § Clear guidelines for EFM observation and interpretation § Standardize maternal fetal record form for each admission

§ Uterine hyperstimulation § Positive culture for group B streptococcus § Placental abruption § Uterine rupture § Preterm labor resulting in unexpected preterm birth § Magnesium sulfate toxicity § Eclampsia § Amniotic fluid embolism § Postpartum hemorrhage § Disseminated intravascular coagulation § Return to the surgical suite after cesarean birth § Admission to the intensive care unit
 § Prolapsed umbilical cord § Vasa")
§ Nonreassuring fetal heart rate pattern (2005 article) § Prolapsed umbilical cord § Vasa previa rupture § Second-stage intolerance to pushing § Shoulder dystocia § Emergent cesarean birth for nonreassuring fetal status § Low Apgar scores at 5 minutes in the term infant § Umbilical cord blood values suggestive of acidemia § Term infant admitted to the special care nursery or neonatal intensive care unit § Subgaleal hematoma

§ Acknowledgment that rescue requires a team effort, although individual providers can contribute significantly to positive outcomes; when an adverse outcome occurs, it is rarely the result of an individual’s action or lack of action. Multiple care providers are involved in the processes that lead to patient harm or injury. When measuring the rescue process, the team’s response is a critical component.

Labor: 80% of the time, Category 2
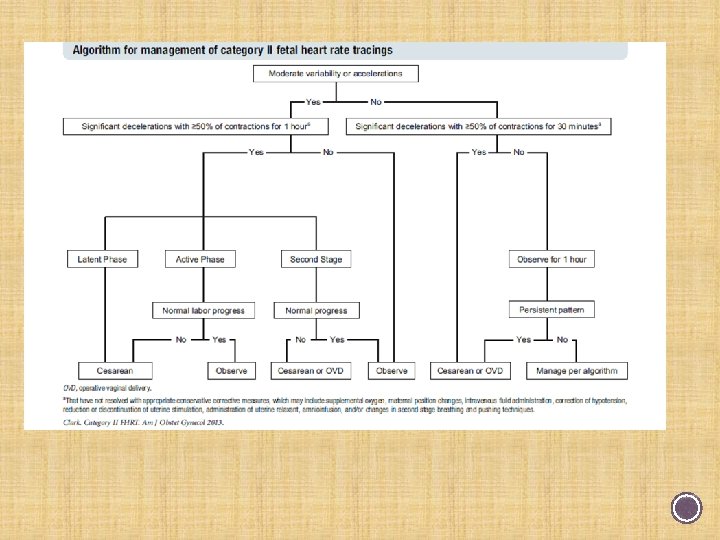

§ Team approach § Common mental model § Stage of labor significant § Normal progress? § Did not address marked variability § Combined minimal and absent

§ Be informed, keep updated § Review current evidence and standards as they are published § Take the initiative to move forward § Be willing to change, then actually do it § Encourage others; be positive § Support the leadership team § Educate women and families

§ Help and hurt § Unbelievable scrutiny § Must accurately reflect occurrence and sequence of events § Purpose: § Facilitate communication between and among caregivers § Promote improved quality of care by encouraging assessment and reevaluation of progress and clinical plans § Meet professional and legal standards

Less than half of well-educated women know the signs and symptoms of preeclampsia. And still others may not share their symptoms with their healthcare providers for fear of over-reacting. Pre eclamptic Foundation

§ Credibility is currency in the courtroom § Assumption is everyone is a good person, once credibility is gone than the case will be lost because the jury gets angry § How you present yourself is very important
- Slides: 42