Julie Caplow May 5 2017 Free Clinic Association





































- Slides: 40
Julie Caplow May 5, 2017 Free Clinic Association of PA Conference
§ Who is a refugee? § Definitions and trends § Services they are entitled to § What do I do if a refugee walks into my clinic? § Screenings recommendations § Health profiles § What can we do better in PA?
Forcibly displaced persons Internally displaced persons Asylum seekers A refugee is a person who owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group, or political opinion, is outside the country of his nationality, and is unable to or, owing to such fear, is unwilling to avail himself of the protection of that country. is unwilling to avail himself of the -1951 Geneva Convention Refugees
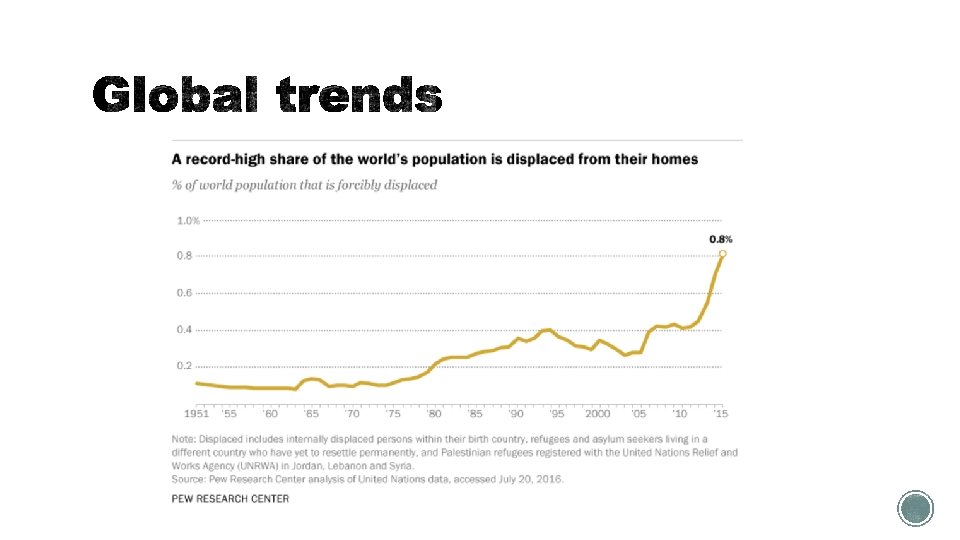
Forcibly displaced persons 65 million Internally displaced persons 40 million Durable solutions: Asylum seekers 3 million Repatriation Refugees 21 million Local integration Resettlement <1% Gobal Trends, 2015 http: //www. unhcr. org/576408 cd 7
Forcibly displaced persons 65 million Internally displaced persons 40 million Durable solutions: Asylum seekers 3 million Repatriation Refugees 50, 000/yr 21 million Local integration Resettlement <1% Gobal Trends, 2015 http: //www. unhcr. org/576408 cd 7
REFUGEE ARRIVALS TO PA, OCT 2015 - SEP 2016 Other § 3679 total arrivals between SYRIA UKRAINE Oct 2015 and Sept 2016 AFGHANISTAN IRAQ BURMA DEM REP OF CONGO CUBAN ENTRANT SOMALIA Pennsylvania Refugee Resettlement Program; http: //www. refugeesinpa. org/aboutus/demoandarrivalstats/index. htm BHUTAN
§ Coordinated by the PA Refugee Resettlement Program, with more than 30 partner organizations § Funded by US Department of Health and Human Services § Each refugee gets paired with a caseworker for the first 3 months of arrival § Services include: § Housing § Health screening § Employment counseling and training § English as a second language § Citizenship preparation
§ Domestic health screening performed within first 30 days of arrival § 10 “refugee clinics” exist in Philadelphia for this purpose § 8 months of insurance coverage under Refugee Medical Assistance § PA Medicaid equivalent § Refugees are then eligible for ACA and Medicaid § Do not have to wait 5 years as other legal immigrants do
Standard overseas and domestic screening
Performed in refugee camp prior to departure § Purpose: “to identify certain disorders that could result in exclusion from the United States under the provisions of the Immigration and Nationality Act. ” § Communicable diseases (TB, syphilis, leprosy) § Mental health disorders § Substance abuse § Criminal behavior § “Public charge grounds” § Also receive empiric treatment of common diseases e. g. intestinal parasites Source: www. cdc. gov/immigrantrefugeehealth
§ Performed within 30 days of arrival in the U. S. § More extensive H&P § Numerous screening tests and immunizations § Stabilization of any acute medical issues § Guidelines specific to country of origin Source: www. cdc. gov/immigrantrefugeehealth
Case comparison: Congolese and Syrian refugee health needs
§Who are they? §What are their health needs?
§ DRC has been in conflict for nearly 2 decades § 1996 -1997 (First Congo War) § 1998 – 2003 (Second Congo War) § 2003 - today: continued human rights abuses, particularly against Congolese of Rwandan origin § Since 2013, more than 400, 000 Congolese fled DRC
Health priorities per the CDC: § Parasitic infections § Malaria § Mental health § Sexual- and gender-based violence https: //www. cdc. gov/immigrantrefugeehealth/pdf/congolesehealth-profile. pdf
• Per CDC, Congelese should be presumptively treated within 3 days of departure from refugee camp • If not, or if symptomatic, screen with thick and thin smear • Treatment: • P. falciparum (90%): Atovaquone-proguanil (Malarone) or artemether-lumefantrine (Coartem)
§ Many are asymptomatic but can have long-term consequences § Schistosomiasis § If untreated, can cause portal hypertension, cirrhosis, urinary obstruction, bladder cancer § Presumptive treatment with praziquantel recommended § Strongyloides § Can cause non-specific GI, skin, pulmonary symptoms; § Hyperinfection syndrome if immunosuppressed § If positive serology, treat with ivermectin § Filaria (e. g. elephantiasis, loa, onchocerciasis) § Test for these if patient has unexplained eosinophilia
§ 40% of Congolese women and 24% of men reported being victims of sexual violence 1 § Resulting high rates of emotional and physical trauma: PTSD, genital fistulas, infertility, HIV/AIDS and other STIs 1 Johnson K et al. Association of Sexual Violence and Human Rights Violations with Physical and Mental Health in Territories of the Eastern Democratic Republic of the Congo. Journal of the American Medical Association 2010; Vol. 304. No. 5: 553 -62
§ <1% reported mental health issues in the pre-departure screening, but close to half of adults met criteria for MDD and PTSD § Group psychotherapy may be more effective than individual psychotherapy § Fuys, Andrew, and Sandra Vines. (2013) “Increasing Congolese Refugee Arrivals: Insights for Preparation. ” Executive Summary. Washington DC: Refugee Council USA. Print. February 15. Report from Associate Directors for International Programs and Resettlement and Integration, Church World Service § Bass JK, Annan J, Murray S et al. Controlled Trial of Psychotherapy for Congolese Survivors of Sexual Violence. N Engl J Med 2013; 368: 2182 - 91.
• Very thorough TB screening overseas very few active cases arrive to the U. S. • However, nearly 1 in 3 have latent TB • High risk of reactivation TB within first year of arrival
§Who are they? §What are their health needs?
§ Largest refugee crisis since WWII § Of a pre-war population of 22 million, half have been displaced § Strong education and health systems prior to the conflict
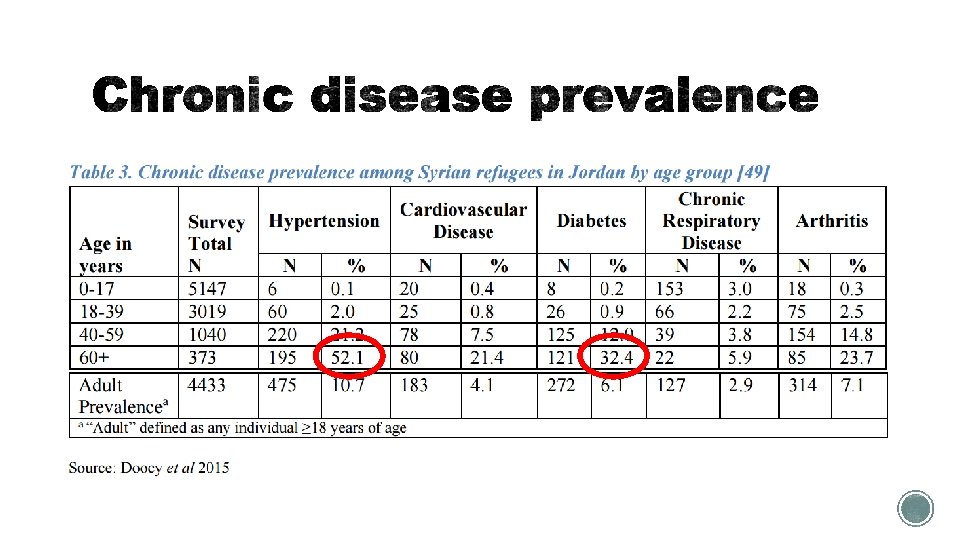
CDC Health Priorities: § Anemia § Hypertension § Diabetes § Mental illness Source: https: //www. cdc. gov/immigrantrefugeehealth
§ High prevalence of anemia in women and children, mostly iron deficiency § Approximately 5% of the Syrian population are carriers of beta thalassemia trait
§ Depression and anxiety very common § Stigmatized in the Syrian community § International Medical Corps, Syria Crisis: Addressing Regional Mental Health Needs and Gaps in the Context of the Syria Crisis. 2015. § Sirin, S. R. and L. Rogers-Sirin, The education and mental health needs of Syrian refugee children. 2015, Migration Policy Institute.
Syrians Congolese Communicable diseases Mental Health Noncommunicable diseases
What can we do better in PA?
Case management by resettlement agency 3 months Health screening and stabilization 1 -4 months Arrival to the U. S. Healthcare coverage under Refugee Medical Assistance 8 months 1 year post-arrival
Survey of refugee patients 1 year after arrival: Health Insurance Status Need a PCP 16% 31% 53% 16% Yes 84% No Unsure Yes No Long-term health access among refugee patients: a needs assessment. Caplow J, Nguyen L, Obidowski J, Barden-Maja A. Poster presentation, Penn Health Equity Week. April 6. 2017.
§ Language is the most commonly identified barrier to refugee care § Refugees may speak obscure dialects – difficult to obtain skilled interpreters § Visits are time-consuming Primary care clinics with language services, courtesy of Penn Service. Link
§ Examples: § Lack of perceived need for preventive health § Alternative medicines and beliefs § Stigmatization of certain health disorders § Lack of awareness of patient confidentiality
§ Mental health services § Difficult to access in Philadelphia § Overwhelming need for dental and eye exams § Women’s health visits § Increased PAP completion with in-person female interpreters § Latent TB treatment § Much improved adherence rates with pharmacy directed treatment monitoring program (40% 94% completion rates!) § Carter KL, Gabrellas AD, Shah S, Garland JM. Improved latent tuberculosis therapy completion rates in refugee patients through use of a clinical pharmacist. Int J Tuberc Lung Dis. 2017 Apr 1; 21(4): 432 -437.
§ The flow of refugees worldwide is at an all-time high § Refugees undergo health screening before and after travel, and have 8 months of insurance coverage via RMA § Refugee health priorities vary vastly depending on their origin § The CDC website is an excellent resource! § Current areas of need: § Long-term insurance coverage and primary care § Interpretation services § Mental health, GYN, dental and vision care
§ Expand network of primary care providers for refugees in PA § Educate about refugee health needs § Increase availability of interpreter services § Contact your local resettlement agencies! § Partner with mental health, GYN, optometry and dental providers § Streamline insurance renewal process after RMA expires
§ UN Refugee Agency: http: //www. unhcr. org § CDC: http: //www. cdc. gov/immigrantrefugeehealth § PA Refugee Resettlement Program: http: //www. refugeesinpa. org § Philadelphia Refugee Health Collaborative: http: //philarefugeehealth. org/
§ Aba Barden, Carol Mc. Laughlin and Kim Carter § HIAS § Penn refugee clinic attendings, residents and student volunteers § Free Clinic Association of PA
Test CBC with diff Quantiferon Gold Hepatitis B s. Ag, s. Ab, c. Ab Whom to test Everyone HIV RPR Urine GC/chlamydia Everyone VZV serology (Ig. G) Everyone Strongyloides Ab Malaria smear Everyone, unless pretreated with Ivermectin Everyone If from Sub-Saharan Africa or h/o malaria or positive symptom screen; not required if pretreated within 3 days of departure Schistosoma Ab African and Middle Eastern patients, unless pretreated with praziquantel B 12 Nepali patients Urine Hcg All women of child-bearing age MMR serologies Pregnant women only CMP, A 1 c, Lipids, Hep C Ab As per US guidelines and provider discretion Immunization Tdap Whom to immunize Everyone - even if already received tetanus MMR Everyone EXCEPT pregnant women VZV Visit #2: Those whom are non-immune, EXCEPT pregnant women Hep B series Visit #2: Those whom are non-immune Influenza Everyone during flu season HPV All men and non-pregnant women <26 years Pneumococcal As per US guidelines (23 and 13 valent) Meningococcal Everyone up to age 19 or going to college/military Polio Ages 18 -25 if attending public school https: //www. cdc. gov/immigrantrefugeehealth/guid elines/domestic-guidelines. html