Journal Club Rawshani A Franzn S Sattar N

Journal Club Rawshani A, Franzén S, Sattar N, Eliasson B, Svensson AM, Zethelius B, Miftaraj M, Mc. Guire DK, Rosengren A, Gudbjörnsdottir S. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2018 Aug 16; 379(7): 633 -644. doi: 10. 1056/NEJMoa 1800256. ASCEND Study Collaborative Group. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N Engl J Med. 2018 Aug 26. doi: 10. 1056/NEJMoa 1804988. 2018年 10月11日 8: 30 -8: 55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi

From the Department of Molecular and Clinical Medicine, Institute of Medicine (Aidin Rawshani, Araz Rawshani, B. E. , A. Rosengren, S. G. ), and the Health Metrics Unit, Sahlgrenska Academy (S. F. ), University of Gothenburg, and the Swedish National Diabetes Register, Center of Registers in Region (Aidin Rawshani, Araz Rawshani, S. F. , B. E. , A. -M. S. , M. M. , S. G. ), Gothenburg, and the Department of Public Health and Caring Sciences–Geriatrics, Uppsala University, and the Swedish Medical Products Agency, Uppsala (B. Z. ) — all in Sweden; the Institute of Cardiovascular and Medical Sciences, University of Glasgow, United Kingdom (N. S. ); and the Division of Cardiology, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas (D. K. M. ). N Engl J Med. 2018 Aug 16; 379(7): 633 -644.

Background Patients with diabetes are at higher risk for death and cardiovascular outcomes than the general population. We investigated whether the excess risk of death and cardiovascular events among patients with type 2 diabetes could be reduced or eliminated.

Methods In a cohort study, we included 271, 174 patients with type 2 diabetes who were registered in the Swedish National Diabetes Register and matched them with 1, 355, 870 controls on the basis of age, sex, and county. We assessed patients with diabetes according to age categories and according to the presence of five risk factors (elevated glycated hemoglobin level, elevated low-density lipoprotein cholesterol level, albuminuria, smoking, and elevated blood pressure). Cox regression was used to study the excess risk of outcomes (death, acute myocardial infarction, stroke, and hospitalization for heart failure) associated with smoking and the number of variables outside target ranges. We also examined the relationship between various risk factors and cardiovascular outcomes.

We defined whether the risk-factor variables were within target ranges on the basis of guideline-recommended target levels. 5, 6 The regression models included the covariable “category, ” which denoted the number of risk-factor variables that were not within the target range (scale, none to five variables). The following five risk factors were considered: 1. the glycated hemoglobin level (cutoff value, ≥ 7. 0% or ≥ 53 mmol per mole), 2. systolic and diastolic blood pressure (cutoff value, ≥ 140 mm Hg for systolic blood pressure or ≥ 80 for diastolic blood pressure), 3. albuminuria (the presence of microalbuminuria or macroalbuminuria), 4. smoking (being a current smoker at study entry), and 5. the LDL cholesterol level (cutoff value, ≥ 2. 5 mmol per liter [97 mg
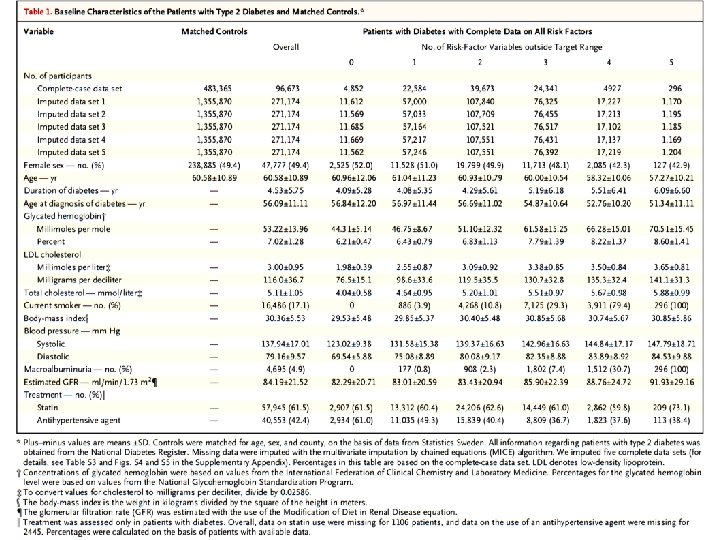

Figure 1. Adjusted Hazard Ratios for Outcomes, According to Age Category and Number of Risk-Factor Variables outside Target Ranges, among Patients with Type 2 Diabetes, as Compared with Matched Controls. Hazard ratios show the excess risk of each outcome among patients with type 2 diabetes, as compared with matched controls from the general population, according to age categories and to the number of risk-factor variables (scale, none to five) that were outside target ranges currently recommended in guidelines. The analysis included patients with type 2 diabetes and controls matched for age, sex, and county in Sweden. We constructed a Cox hazards model for each age category, and these models were adjusted for the covariable “category”; this covariable denotes the number of risk-factor variables that were within target ranges. These Cox model analyses were performed on five imputed data sets for each age category, elevated glycated hemoglobin elevated low-density lipoprotein and hazard ratioslevel, were pooled from all cholesterol level, albuminuria, smoking, and elevated blood pressure the data sets with the use of Rubin’s rule.

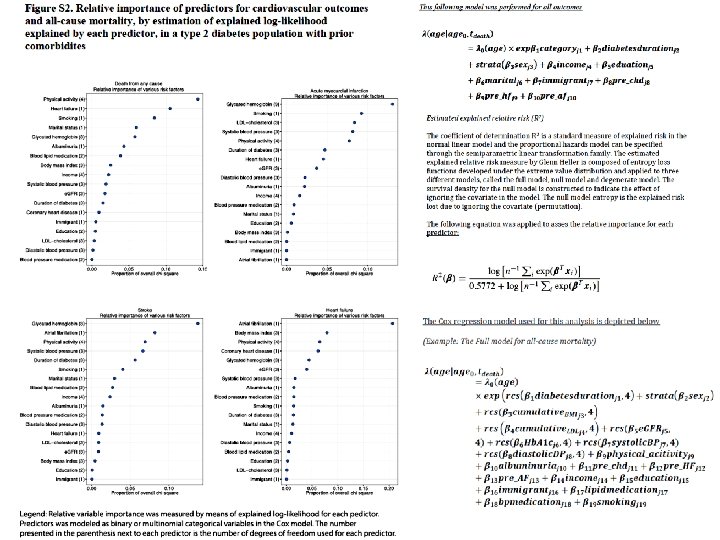
Figure 2. Relative Importance of Risk Factors for Predicting Death from Any Cause, Acute Myocardial Infarction, Stroke, and Hospitalization for Heart Failure among Patients with Type 2 Diabetes, with or without Preexisting Conditions. The estimated explained relative risk (i. e. , relative importance) shows the strength of the association for various risk-factor variables (with values outside the target ranges) for predicting death (Panel A), acute myocardial infarction (Panel B), stroke (Panel C), and hospitalization for heart failure (Panel D) among patients with type 2 diabetes. Results were obtained from the first imputed data set; there were no significant differences between the sets. The analysis was restricted to patients with type 2 diabetes. We constructed a Cox hazard model for each outcome, which included every predictor. We then constructed a separate Cox model for each predictor and permutated covariables from each of these Cox models to estimate the explained relative risk (R 2). R 2 was generated by developed applications for the Cox model and is bounded between 0 and 1. Risk factors showing a clear and substantial R 2 measure, as compared with other adjacent predictors, are considered to be relevant. Full definitions of the risk factors and the values that were considered to be outside the target ranges are provided in the Supplementary Appendix. The body-mass index is the weight in kilograms divided by the square of the height in meters. LDL

Figure 2. Relative Importance of Risk Factors for Predicting Death from Any Cause, Acute Myocardial Infarction, Stroke, and Hospitalization for Heart Failure among Patients with Type 2 Diabetes, with or without Preexisting Conditions. The estimated explained relative risk (i. e. , relative importance) shows the strength of the association for various risk-factor variables (with values outside the target ranges) for predicting death (Panel A), acute myocardial infarction (Panel B), stroke (Panel C), and hospitalization for heart failure (Panel D) among patients with type 2 diabetes. Results were obtained from the first imputed data set; there were no significant differences between the sets. The analysis was restricted to patients with type 2 diabetes. We constructed a Cox hazard model for each outcome, which included every predictor. We then constructed a separate Cox model for each predictor and permutated covariables from each of these Cox models to estimate the explained relative risk (R 2). R 2 was generated by developed applications for the Cox model and is bounded between 0 and 1. Risk factors showing a clear and substantial R 2 measure, as compared with other adjacent predictors, are considered to be relevant. Full definitions of the risk factors and the values that were considered to be outside the target ranges are provided in the Supplementary Appendix. The body-mass index is the weight in kilograms divided by the square of the height in meters. LDL

IFCC 53 64 75 100 150 NGSP 7. 0 8. 0 9. 0 11. 3 15. 9 IFCC(mmol/mol)= 10. 93×NGSP(%)− 23. 52 7. 0% Figure 3. Association between Levels of Glycated Hemoglobin, Systolic Blood Pressure, and LDL Cholesterol and Death from Any Cause, Acute Myocardial Infarction, Stroke, and Heart Failure in Patients with Type 2 Diabetes. We constructed a Cox model for each outcome and applied a prediction function to assess the relationship between glycated hemoglobin, systolic blood-pressure, and LDL cholesterol levels and the risks of death from any cause (Panel A), acute myocardial infarction (Panel B), stroke (Panel C), and hospitalization for heart failure (Panel D). Reference values were the contemporary guideline levels: 53 mmol per mole for the glycated hemoglobin level, 140 mm Hg for the systolic blood pressure, and 2. 5 mmol per liter (97 mg per deciliter) for the LDL cholesterol level. The dark lines indicate the hazard function, and the shaded areas 95% confidence intervals. Continuous variables were modeled with restricted cubic splines, whereas all the categorical variables were

Results The median follow-up among all the study participants was 5. 7 years, during which 175, 345 deaths occurred. Among patients with type 2 diabetes, the excess risk of outcomes decreased stepwise for each risk-factor variable within the target range. Among patients with diabetes who had all five variables within target ranges, the hazard ratio for death from any cause, as compared with controls, was 1. 06 (95% confidence interval [CI], 1. 00 to 1. 12), the hazard ratio for acute myocardial infarction was 0. 84 (95% CI, 0. 75 to 0. 93), and the hazard ratio for stroke was 0. 95 (95% CI, 0. 84 to 1. 07). The risk of hospitalization for heart failure was consistently higher among patients with diabetes than among controls (hazard ratio, 1. 45; 95% CI, 1. 34 to 1. 57). In patients with type 2 diabetes, a glycated hemoglobin level outside the target range was the strongest predictor of stroke and acute myocardial infarction; smoking was the strongest predictor of death.

Conclusions Patients with type 2 diabetes who had five riskfactor variables within the target ranges appeared to have little or no excess risk of death, myocardial infarction, or stroke, as compared with the general population. (Funded by the Swedish Association of Local Authorities and Regions and others. )


The affiliations of the members of the writing committee are as follows: Clinical Trial Service Unit and Epidemiological Studies Unit, Nuffield Department of Population Health (L. B. , M. M. , K. W. , W. S. , G. B. , J. Barton, K. M. , R. H. , J. C. , A. M. , A. Y. , M. L. , F. C. , E. S. , E. W. , D. S. , R. P. , C. B. , R. C. , S. P. , J. A. ), Nuffield Department of Primary Care Health Sciences (A. F. ), and Wolfson College (A. N. ), University of Oxford, the Royal Berkshire NHS Foundation Trust, Reading (T. A. ), Addenbrooke’s Hospital, Cambridge (A. A. ), Leeds General Infirmary, Leeds (J. Bodansky), and University Hospital of Wales, Cardiff (R. M. ) — all in the United Kingdom. N Engl J Med. 2018 Aug 26. doi: 10. 1056/NEJMoa 1804988.

Background Diabetes mellitus is associated with an increased risk of cardiovascular events. Aspirin use reduces the risk of occlusive vascular events but increases the risk of bleeding; the balance of benefits and hazards for the prevention of first cardiovascular events in patients with diabetes is unclear.

Methods We randomly assigned adults who had diabetes but no evident cardiovascular disease to receive aspirin at a dose of 100 mg daily or matching placebo. The primary efficacy outcome was the first serious vascular event (i. e. , myocardial infarction, stroke or transient ischemic attack, or death from any vascular cause, excluding any confirmed intracranial hemorrhage). The primary safety outcome was the first major bleeding event (i. e. , intracranial hemorrhage, sight-threatening bleeding event in the eye, gastrointestinal bleeding, or other serious bleeding). Secondary outcomes included gastrointestinal tract cancer.

* Plus–minus values are means ±SD. Numbers and percentages are shown for categorical variables, and means or medians (with interquartile ranges) for continuous variables. There were no significant differences between the assigned groups. Percentages may not total 100 because of rounding. † Race and ethnic group were reported by the participant. Other groups were Indian, Pakistani, or Bangladeshi (1% of participants), African or Caribbean (1%), and other or unknown (1%). ‡ The body-mass index (the weight in kilograms divided by the square of the height in meters) was based on values for height and weight that were reported by the participants. § The presence of type 2 diabetes was based on a broad clinical definition involving the age of the participant at the diagnosis of diabetes, the use of insulin within 1 year after diagnosis, and the bodymass index. ¶ We categorized the predicted 5 -year risk of serious vascular event (including transient ischemic attack) without the use of aspirin or n− 3 fatty acids as follows: low risk as less than 5%, moderate risk as 5% to less than 10%, and high risk as 10% or more.
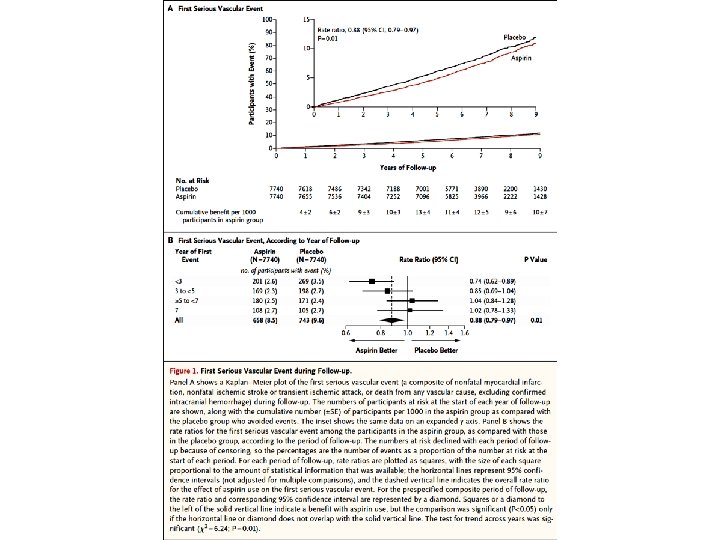

Figure 2. Effect of Assignment to Aspirin Group on Components of Serious Vascular Events, the Combined Outcome of Serious Vascular Event or Revascularization, and Major Bleeding and Its Components. The primary outcome was a serious vascular event (a composite of nonfatal myocardial infarction, nonfatal ischemic stroke or transient ischemic attack [TIA], or death from any vascular cause, excluding confirmed intracranial hemorrhage). Secondary outcomes were a serious vascular event or any coronary or noncoronary revascularization procedure. A single participant may have had multiple events and therefore may contribute information to more than one row. The size of each square for the ratio is proportional to the amount of statistical information that was available, the horizontal lines represent 95% confidence intervals, and the dashed vertical line indicates the overall rate ratio for the effect of aspirin use on the first serious vascular event. An arrow on the horizontal line indicates that the confidence interval exceeds the graph area. For composite outcomes, rate ratios and their corresponding 95% confidence intervals are represented by diamonds. Bold entries with diamonds show totals for all data listed above them. The effect of aspirin use on the components of the primary safety outcome of major bleeding event (a composite of intracranial hemorrhage, sightthreatening bleeding event in the eye, gastrointestinal bleeding, or other major
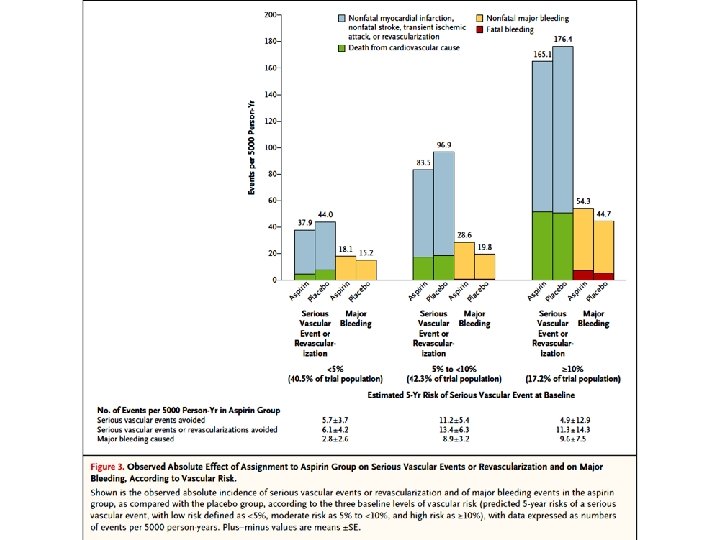
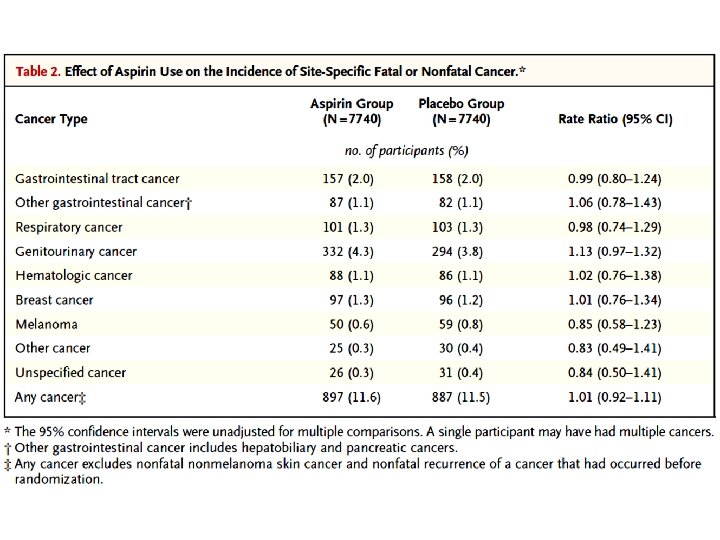

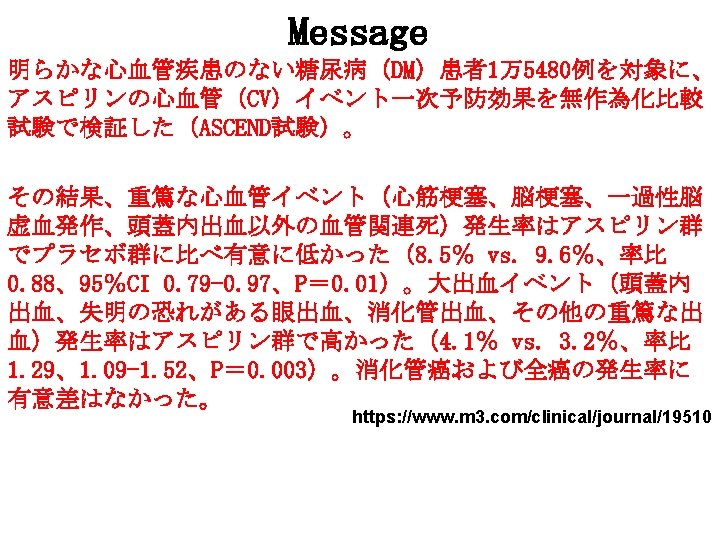
Results A total of 15, 480 participants underwent randomization. During a mean follow-up of 7. 4 years, serious vascular events occurred in a significantly lower percentage of participants in the aspirin group than in the placebo group (658 participants [8. 5%] vs. 743 [9. 6%]; rate ratio, 0. 88; 95% confidence interval [CI], 0. 79 to 0. 97; P=0. 01). In contrast, major bleeding events occurred in 314 participants (4. 1%) in the aspirin group, as compared with 245 (3. 2%) in the placebo group (rate ratio, 1. 29; 95% CI, 1. 09 to 1. 52; P=0. 003), with most of the excess being gastrointestinal bleeding and other extracranial bleeding. There was no significant difference between the aspirin group and the placebo group in the incidence of gastrointestinal tract cancer (157 participants [2. 0%] and 158 [2. 0%], respectively) or all cancers (897 [11. 6%] and 887 [11. 5%]); long-term follow-up for these outcomes is planned.

Conclusions Aspirin use prevented serious vascular events in persons who had diabetes and no evident cardiovascular disease at trial entry, but it also caused major bleeding events. The absolute benefits were largely counterbalanced by the bleeding hazard. (Funded by the British Heart Foundation and others; ASCEND Current Controlled Trials number, ISRCTN 60635500; Clinical. Trials. gov number, NCT 00135226. )

- Slides: 27