Journal Club Elisa De Franco Sarah E Flanagan

Journal Club Elisa De Franco, Sarah E Flanagan, Jayne AL Houghton, Hana Lango Allen, Deborah JG Mackay, I Karen Temple, Sian Ellard, Andrew T Hattersley The effect of early, comprehensive genomic testing on clinical care in neonatal diabetes: an international cohort study Lancet, July 29, 2015. Melanie J. Davies, MD; Richard Bergenstal, MD; Bruce Bode, MD; Robert F. Kushner, MD; Andrew Lewin, MD; Trine Vang Skjøth, MD; Arne Haahr Andreasen, MSc; Christine Bjørn Jensen, MD; Ralph A. De. Fronzo, MD Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes The SCALE Diabetes Randomized Clinical Trial JAMA. 2015; 314(7): 687 -699. doi: 10. 1001/jama. 2015. 9676 2015年 9月03日 8: 30 -8: 55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University Sellami Mnif Houda


MODY http: //www. diabetesgenes. org/content/mody-probability-calculator HNF 1 A Glucokinase HNF 4 A Renal Cysts & Diabetes (HNF 1 B) Neonatal Diabetes KIR 6. 2/SUR 1 (KCNJ 11 ABCC 8) Sulfonylurea therapy! 2型糖尿病の病態に関連する遺伝子 Nat Genet. 2012 Sep; 44(9): 981 -90.

Article The effect of early, comprehensive genomic testing on clinical care in neonatal diabetes: an international cohort study Elisa De Franco, Sarah E Flanagan, Jayne AL Houghton, Hana Lango Allen, Deborah JG Mackay, I Karen Temple, Sian Ellard, Andrew T Hattersley Institute of Biomedical and Clinical Science, University of Exeter Medical School, Exeter, UK (E De Franco Ph. D, S E Flanagan Ph. D, J A L Houghton Ph. D, H Lango Allen Ph. D, Prof S Ellard Ph. D, Prof A T Hattersley DM) ; Wessex Regional Genetics Laboratory, Salisbury Foundation Trust, Salisbury, UK (D J G Mackay Ph. D, Prof I K Temple MD) ; University Hospital Southampton NHS Trust, Southampton, UK (D J G Mackay, Prof I K Temple) ; and Human Genetics and Genomic Medicine, Faculty of Medicine, University of Southampton, UK (D J G Mackay) Lancet. July 29, 2015
 is changing Improved sequencing")
Traditional genetic testing (analysis of one or a few genes) is changing Improved sequencing methods enable simultaneous analysis of several genes. . Genetic subtype (Neonatal diabetes) defines treatment, with improved glycaemic control on sulfonylurea treatment for most patients with potassium channel mutations. TARGET To investigated the effect of early, comprehensive testing of all known genetic causes of neonatal diabetes.

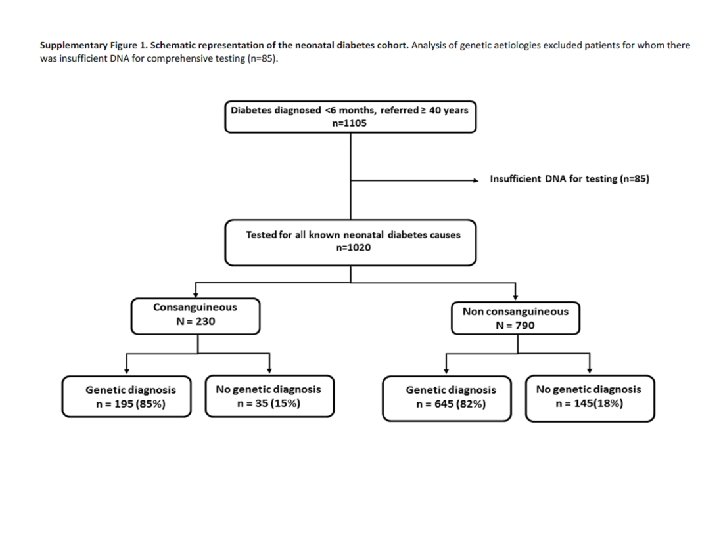
Methods -Large, international, cohort study, - patients with neonatal diabetes diagnosed with diabetes before 6 months of age -From 79 countries. - Mutations were identified by comprehensive genetic testing including Sanger sequencing, 6 q 24 methylation analysis, and targeted next-generation sequencing of all known neonatal diabetes genes.

Supplementary Table 2. Number and references for 253 patients included in the cohort who have been included inprevious publications by the Exeter team.

PLAGL 1 ? Supplementary Table 3. Genetic causes of neonatal diabetes identified in 840 neonatal diabetes patients.
![RESULTS: - Recessive causes were common (158 [81%] of 195 patients) in the off](http://slidetodoc.com/presentation_image_h/17299d9a4348db4293c6c32c464056f7/image-11.jpg "RESULTS: - Recessive causes were common (158 [81%] of 195 patients) in the off")
RESULTS: - Recessive causes were common (158 [81%] of 195 patients) in the off spring of consanguineous parents but unusual (81 [13%] of 645 patients) when the parents were not consanguineous (p<0・ 0001; df=1). -The major genetic cause differed depending on whether the parents were related - Mutations in the INS gene were present at a similar proportion in the two group - In non-consanguineous group, most INS gene mutations were heterozygous 46% p<0· 0001 12%

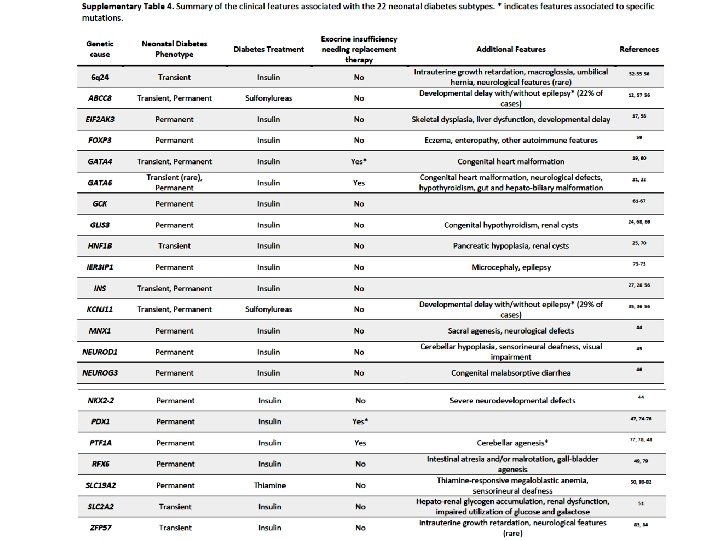
The pancreatic phenotypes include: - Transient neonatal diabetes (6 q 24, ABCC 8, KCNJ 11, INS, HNF 1 B, SLC 2 A 2, ZFP 57 subtypes), in which the diabetes resolves -Permanent diabetes responding to sulfonylurea treatment (KCNJ 11 and ABCC 8) - Permanent insulin-treated diabetes (INS, GCK, EIF 2 AK 3, FOXP 3, GLIS 3, NEUROD 1, NEUROG 3, NKX 2 -2, MNX 1, IER 3 IP 1, RFX 6, and some cases with GATA 6, GATA 4 and PDX 1 mutations) - Developmental disorders of the exocrine pancreas (GATA 6, PTF 1 A, PDX 1 and GATA 4) requiring pancreatic enzyme replacement in addition to insulin treatment - Diabetes caused by SLC 19 A 2 gene mutations can sometimes be successfully treated with thiamine. the identification of the genetic cause defines the treatment requirements for the endocrine and exocrine pancreatic function Specific extra-pancreatic features (neurological features) are being the most common (n=184). Mutations in nine genes (ABCC 8 [22% of cases], KCNJ 11 [29% of cases], EIF 2 AK 3, SLC 19 A 2, IER 3 IP 1, PTF 1 A, NEUROD 1, MNX 1, and NKX 22) cause neonatal diabetes with neurological abnormalities. generally become evident in infancy, after diagnosis of neonatal diabetes; therefore, early genetic diagnosis in these patients predicts future development of neurological complications. The different genetic causes of neonatal diabetes identified so far have a range of both pancreatic and extra-pancreatic phenotypes

The median time from the diagnosis of diabetes to referral for genetic testing showed a marked decrease from more than 4 years (240 weeks, IQR 218– 4099) in 2004, to less than 3 months (10 weeks, IQR 3– 23) since 2012 The number of referrals per year was steady during the past 10 years at 80– 100 per year Patients with a genetic diagnosis of transient neonatal diabetes caused by 6 q 24 methylation defects or potassium channel gene mutations : Patient’s diabetes had remitted before referral was dependent on the time from diagnosis to genetic testing; only 10 (10%) of 101 patients tested early (48 months after diagnosis) had entered remission when genetic testing was done (p <0· 0001 ) (A) Effect of early genetic diagnosis in transient neonatal diabetes caused by 6 q 24 methylation defects or potassium channel gene mutations. Bar chart representing clinical features at the time of genetic testing for neonatal diabetes. Orange=diabetes, purple=diabetes remitted.

Wolcott-Rallison syndrome is caused by biallelic mutations in EIF 2 AK 3, a gene known to be important for regulation of endoplasmic reticulum stress (DG: the presence of insulin-dependent diabetes and skeletal dysplasia or liver dysfunction) Diabetes diagnosed in the first 6 months of life : skeletal dysplasia is not evident until the infant is 1 or 2 years of age and liver dysfunction generally manifests during intercurrent illness as recurrent episodes of acute liver failure which can present at any time after the neonatal diabetes The non-diabetes features were present only in 3 (12%) of 26 patients with early referral (48 months from diagnosis of diabetes; p <0· 0001 (B) The effect of age at genetic testing on whether patients have non-diabetes features of Wolcott-Rallison Syndrome at the time of referral for genetic testing. Bar chart representing clinical features at the time of genetic testing for neonatal diabetes. Orange=diabetes only, light blue=diabetes and either skeletal abnormalities or liver dysfunction, dark blue=diabetes, skeletal abnormalities, and liver dysfunction.

Specific mutations in KCNJ 11 and ABCC 8 cause a syndromic form of neonatal diabetes characterised by severe development delay and neurological features (DEND [Developmental delay, Epilepsy and Neonatal Diabetes] and i. DEND syndrome) Neurological features were not present in any of the patients with early referral (0 of 7 referred 48 months from diagnosis of diabetes, p<0· 0001 ) (C) The effect of age at genetic testing on whether patients with a KCNJ 11 p. Val 59 Met mutation have neurological features at the time of referral for genetic testing. Bar chart representing clinical features at the time of genetic testing for neonatal diabetes. Orange=diabetes only, green=diabetes and neurological features

CONCLUSION This study describes the transformation that can occur in clinical practice once genetic testing becomes the initial investigation. Traditionally, genetic testing was used to confirm a clinical diagnosis based on disease course or a cluster of clinical features. Now, early comprehensive genetic testing gives a diagnosis before the development of specific features The future of care in neonatal diabetes will increasingly rely on the results of genetic testing with the genetic diagnosis, not only informing a clinician of the likely course and best treatment for the diabetes, but also predicting development of additional clinical features. This model represents a new framework in which genetic testing defi nes, rather than just confirms, the clinical diagnosis.


Reviewed on 20091029 Astrup A, Rössner S, Van Gaal L, Rissanen A, Niskanen L, Al Hakim M, Madsen J, Rasmussen MF, Lean ME; NN 8022 -1807 Study Group. : Effects of liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet. 2009 Nov 7; 374(9701): 1606 -16. doi: 10. 1016/S 0140 -6736(09)61375 -1.
: 11 -22.")
SCALE Obesity and Prediabetes N Engl J Med. 2015 Jul 2; 373(1): 11 -22. doi: 10. 1056/NEJMoa 1411892. Figure 1. Liraglutide and Body Weight. Panel A shows the mean body weight for patients in the fullanalysis set who completed each scheduled visit, according to presence or absence of prediabetes at screening. I bars indicate standard error, and the separate symbols above the curves represent the 56 - week weight change using lastobservation-carried-forward (LOCF) imputation. The fullanalysis set comprised patients who underwent randomization, were exposed to at least one treatment dose, and had at least one assessment after baseline (69 patients were excluded from the full-analysis set: 61 owing to lack of an assessment and 8 owing to no exposure). Panel B shows the proportions of patients who lost at least 5%, more than 10%, and more than 15% of their baseline body weight. Data shown are the observed means for the full-analysis set (with LOCF). Findings from logistic- regression analysis showed an odds ratio of 4. 8 (95% confidence interval [CI], 4. 1 to 5. 6) for at least 5% weight loss and an odds ratio of 4. 3 (95% CI, 3. 5 to 5. 3) for more than 10% weight loss; the analysis of more than 15% weight loss was performed post hoc (odds ratio, 4. 9 [95% CI, 3. 5 to 6. 7]). Panel C shows the cumulative percentage of patients with those changes in body weight after 56 weeks of treatment.

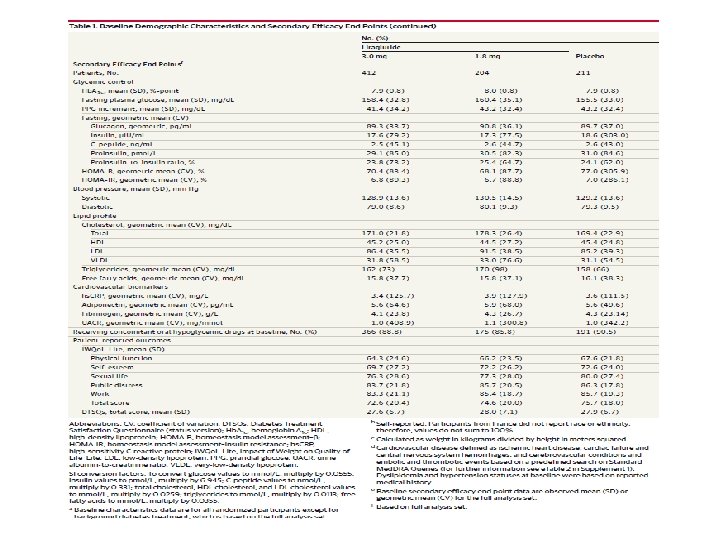
Article Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes The SCALE Diabetes Randomized Clinical Trial Melanie J. Davies, MD; Richard Bergenstal, MD; Bruce Bode, MD; Robert F. Kushner, MD; Andrew Lewin, MD; Trine Vang Skjøth, MD; Arne Haahr Andreasen, MSc; Christine Bjørn Jensen, MD; Ralph A. De. Fronzo, MD; 1 Diabetes Research Centre, University of Leicester, United Kingdom Diabetes Center, Park Nicollet Health Services, Minneapolis, Minnesota 3 Atlanta Diabetes Associates, Atlanta, Georgia 4 Northwestern University, Chicago, Illinois 5 National Research Institute, Los Angeles, California 6 Novo Nordisk A/S, Søborg, Denmark 7 Texas Diabetes Institute, San Antonio 2 International JAMA. 2015; 314(7): 687 -699. doi: 10. 1001/jama. 2015. 9676

- Weight loss is recommended for patients with type 2 diabetes. -Moderate weight loss (5%-10%) can improve glycemic control and other cardiometabolic risk factors and comorbidities. - Liraglutide : analog of the incretin hormone (GLP-1), a unique therapeutic potential for both obesity and type 2 diabetes owing to its dual benefits on body weight and glycemic control. TARGET: To study the efficacy and safety of liraglutide (3. 0 mg), as an adjunct to diet and exercise, for weight management in participants who : 1 - were overweight or obese 2 - had type 2 diabetes

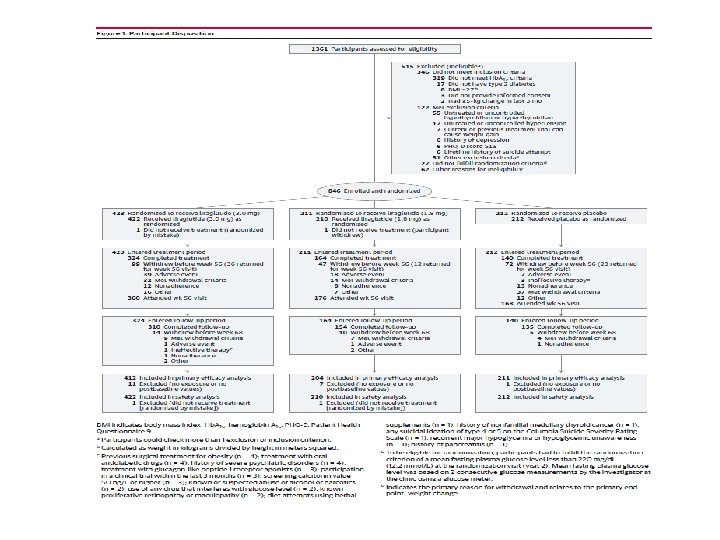
METHODS: 56–week randomized double-blind, placebo controlled, parallel-group trial with 12 -week observational off-drug follow -up period. Study conducted at 126 sites in 9 countries between June 2011 and January 2013. 1361 Elligible patients 846 were randomized. Inclusion criteria: 1 -Body mass index of 27. 0 or greater 2 -Age 18 years or older 3 -Taking 0 to 3 oral hypoglycemic agents (metformin, thiazolidinedione, sulfonylurea) 4 -Stable body weight, and glycated hemoglobin level 7 -10%
 to Group liraglutide (3.")
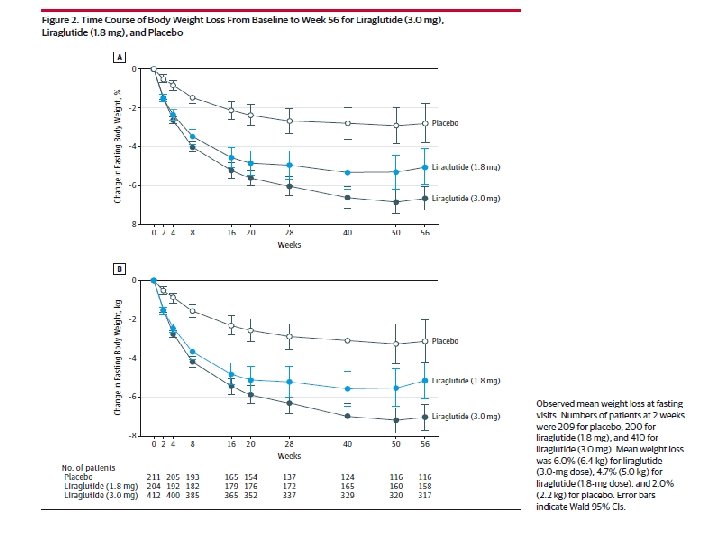
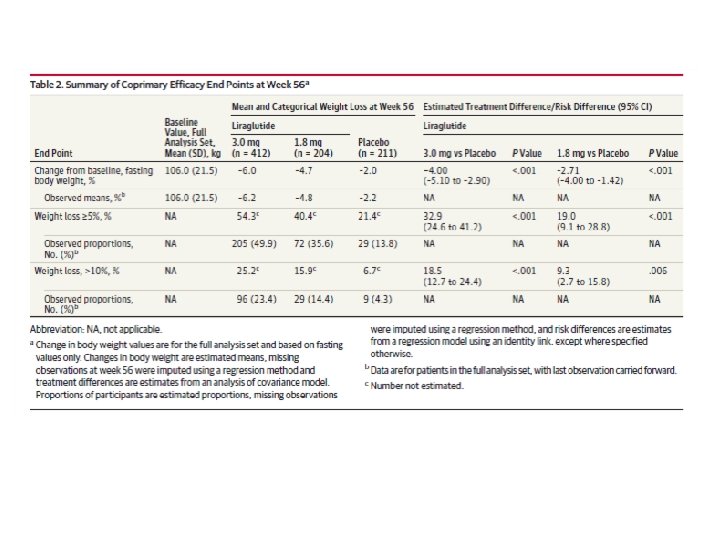
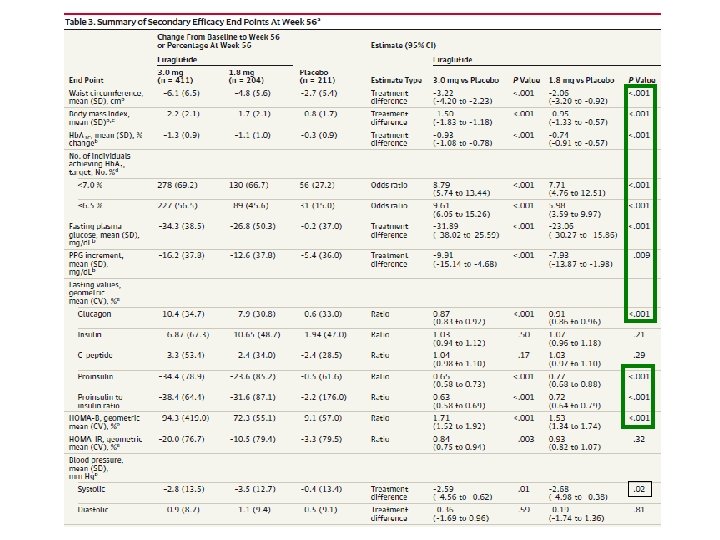
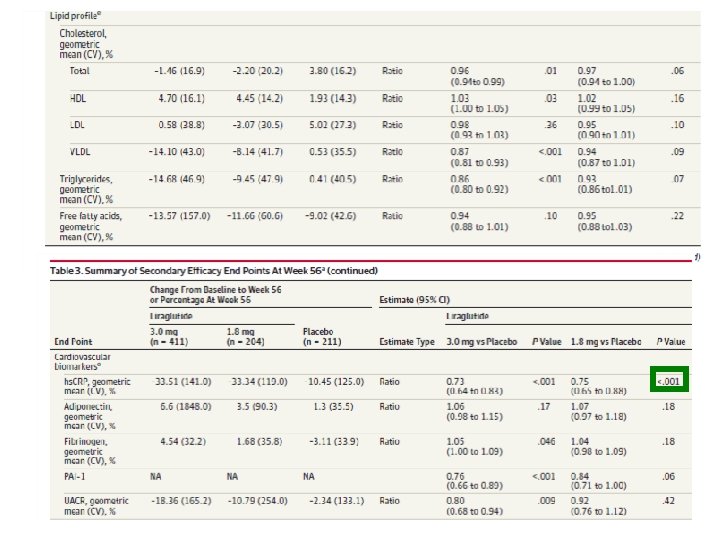
Participants were randomly assigned (in a blinded fashion; week 0) to Group liraglutide (3. 0 mg); Or Group liraglutide (1. 8 mg); or placebo in a 2: 1: 1 ratio. Three coprimary end points at week 56: (1)relative change in bodyweight; (2)the proportion of participants losing 5% or more of baseline body weight; (3)proportion losing more than 10% of baseline bodyweight. Secondary efficacy end points included changes at week 56 in waist circumference, BMI, Hb. A 1 c level, prandial plasma glucose increment

RESULTS


No cases of acute pancreatitis were reported

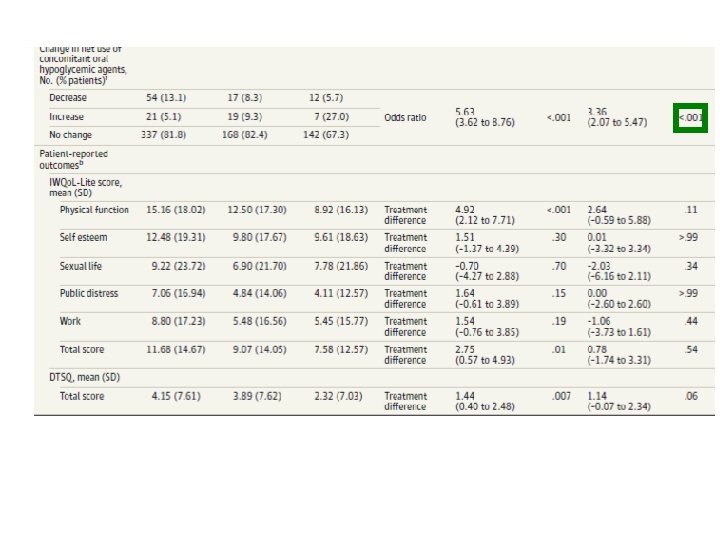
In the present trial, Few severe hypoglycemic episodes were reported (5 with liraglutide [3. 0 mg], 3 with liraglutide [1. 8 mg]), all in participants receiving concomitant sulfonylurea therapy. Measures of weight-related quality of life were significantly improved with liraglutide (3. 0 mg) but not liraglutide (1. 8 mg), primarily driven by a significant improvement in participants’ physical function. Exploratory comparisons between the 2 doses of liraglutide showed that liraglutide (3. 0 mg) was statistically significantly better than liraglutide (1. 8 mg) on all weight- and glycemic-related end points; the difference between the 3. 0 -mg dose and the 1. 8 -mg dose in reduction of Hb. A 1 c level, while statistically significant, was small (0. 19%), but the 3. 0 -mg dose did lead to a larger reduction in participants’ use of oral hypoglycemic agents compared with liraglutide (1. 8 mg). The present study had several limitations. It was not powered to enable conclusions about safety

Conclusion: Among overweight and obese participants with type 2 diabetes, use of subcutaneous liraglutide (3. 0 mg) daily, compared with placebo, resulted in weight loss over 56 weeks. Further studies are needed to evaluate longer-term efficacy and safety.

- Slides: 38