Joint hospital Surgical Grand Round Application of ICG

 spectrum")
 has been used in : ophthalmic angiography determining cardiac")
 has been used in : ophthalmic angiography determining cardiac")


 figures of esophagectomy 09 -10 10 -11 11 -12 12 -13")
 figures of esophagectomy 09 -10 10 -11 11 -12 12 -13")




")
")

 18/40 -ve")































- Slides: 48
Joint hospital Surgical Grand Round Application of ICG in esophagectomy Dr Lim Delon
Introduction ICG a fluorophore that absorbed and emitted light in the near-infrared (NIR) spectrum NIR probe hydrodynamic diameter of 1. 2 nm very small only NIR probe approved by the US Food and Drug Administration (FDA); Methylene blue another FDA-approved probe not considered a pure NIR probe. Karol Polom et al, Current Trends and Emerging Future of Indocyanine Green Usage in Surgery and Oncology, Cancer, 2010
Introduction ICG (NIR fluorescence imaging) has been used in : ophthalmic angiography determining cardiac output and hepatic function New domains: Surgical oncology SLN mapping (eg breast, gastric cancer, etc) Tumor identification Lymphedema and assessment of tissue perfusion Current Trends and Emerging Future of Indocyanine Green Usage in Surgery and Oncology: An Update, Ann Surg Oncol (2015) 22: S 1271–S 1283
Introduction ICG (NIR fluorescence imaging) has been used in : ophthalmic angiography determining cardiac output and hepatic function New domains: Surgical oncology SLN mapping (eg breast, gastric cancer, etc) Tumor identification Lymphedema and assessment of tissue perfusion Current Trends and Emerging Future of Indocyanine Green Usage in Surgery and Oncology: An Update, Ann Surg Oncol (2015) 22: S 1271–S 1283
Introduction Assessment of tissue perfusion Reconstructive surgery Assessment of microvascular circulation of anastomotic site NIR fluorescence made visible with imaging technologies Injected intravenously during operation
Introduction
Introduction Local (HA) figures of esophagectomy 09 -10 10 -11 11 -12 12 -13 13 -14 14 -15 No of cases 141 102 97 98 98 99 30 -day crude mortality(%) 4. 3 1. 0 6. 2 3. 1 1 1 30 -day crude morbidity(%) 62. 4 58. 8 53. 6 57. 1 68. 4 48. 5 Mean anastomotic leak(%) 13. 5 12. 7 7. 2 9. 2 0 6. 1 SOMIP database
Introduction Local (HA) figures of esophagectomy 09 -10 10 -11 11 -12 12 -13 13 -14 14 -15 No of cases 141 102 97 98 98 99 30 -day crude mortality(%) 4. 3 1. 0 6. 2 3. 1 1 1 30 -day crude morbidity(%) 62. 4 58. 8 53. 6 57. 1 68. 4 48. 5 Mean anastomotic leak(%) 13. 5 12. 7 7. 2 9. 2 0 6. 1 SOMIP database
Introduction Anastomotic leakage: important cause of postoperative morbidity and increased length of stay Factors associated with leak low flow or inadequate perfusion of the surgical site procedure duration greater than 5 hours type of procedure obesity, heart failure, coronary disease, vascular disease, hypertension, steroids, diabetes, renal insufficiency, tobacco use Edmund S. Kassis et al, Predictors of Anastomotic Leak After Esophagectomy: An Analysis of The Society of Thoracic Surgeons General Thoracic Database, Ann Thorac Surg 2013; 96: 1919– 26
STUDY
2008 -2011, 40 patients cervical or thoracic esophagectomy ICG fluorescence was detected by a camera and recorded
Results
Results ICG (microcirculation in the stump)
ICG Fluorescence was easily detect intra-operatively in all patients (microcirculation atin 1 the minstump) after ICG injection Results
Results
Results ICG (small vessels in the stump) 18/40 -ve
Results 3 out of 40 anastomotic leak Retrospectively: Small vessels were not observed in the stump of the reconstructive organ’s wall in 18 cases All the leakage cases belong to this group
Conclusion? Imaging of ICG fluorescence May be helpful in evaluating the blood supply of reconstructed organs Microcirculation detected by ICG intraop == provide enough blood flow to maintain a viable anastomosis. Additional and larger study is needed.
Other studies N=20 gastric pullup Conclusions: ICG has potential usefulness for evaluation of blood flow in the gastric tube N=33 thoracic esophagectomy Conclusions: ICG fluorescence can be used to evaluate blood supply
2008 -2011 N = 150 undergoing esophagectomy with gastric pull-up
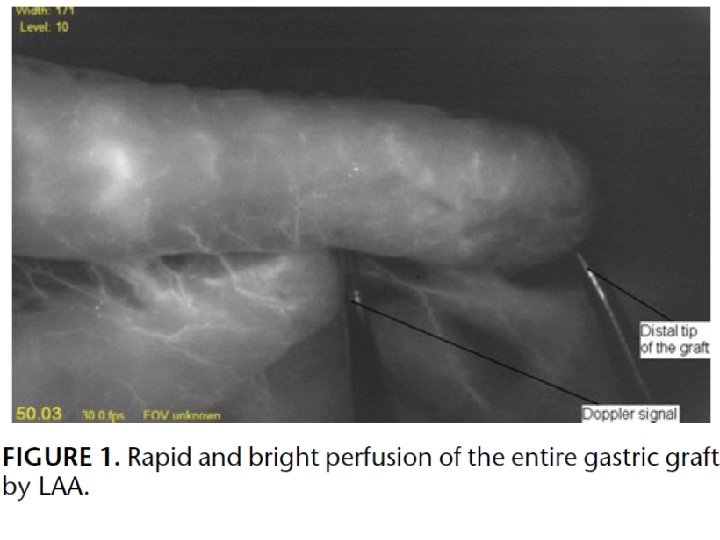
Real-time intraop perfusion assessment by ICG before bringing the graft up through the mediastinum Fluorescence images of the graft captured using a charge coupled device video camera system
Method Transition site from Rapid & bright slow & less robust perfusion Marked with suture The location of the anastomosis relative to the suture compared with leakage rate Outcome measurement: Anastomotic leakage detected by videoesophagram or by upper endoscopy POD 5 -7
VIDEO
Result Transition point +ve: 66% Overall leakage rate: 16. 7%
Result Anastomosis at/distal to suture significantly a/w leak
Result
Result Multivariate analysis: Anastomosis at or distal to suture the only significant factor associated with a leak
Conclusion The use of ICG may lead to an altered surgical plan in some patients and contribute to reduced anastomotic morbidity and better overall patient outcomes Intraop real-time assessment of perfusion correlated with the likelihood of an anastomotic leak
Conclusion Anastomosis was unlikely to leak in patients with no transition point or At proximal to the transition point when present When anastomosis had to be placed at or distal to a transition point ~50% chance of leak should be monitored closely planned graft evaluation on POD 5 -7
Limitation Evaluation of the images is largely qualitative Overall small number of leaks prohibited an evaluation of the impact of operative approach on anastomotic healing masked the role of important comorbid conditions that contribute to leaks Quantitative assessment?
Summary Anastomotic leakage is an important cause of postop morbidity/mortality in esophagectomy Tissue perfusion is one of the important factors affecting leakage rate
Summary ICG is a safe, feasible way to assess perfusion and can potentially affect surgical decision High cost (machine costs ~1 mil HKD) More studies needed Role of quantitative measurement
Other Problems Universal application/ Selection criteria? Training of staff? Resources/ Cost-effectiveness? Clear and non-ambiguous guideline? More evidence and research is needed
THE FUTURE OF ICG? ?
Future of ICG Sentinel LN biopsy in esophageal cancer? Controversial Problems with multidirectional, complicated lymphatic flow ? use in early superficial disease LN dissection during esophagectomy Yasuhiro et al. Sentinel Lymph Node Biopsy Using Intraoperative Indocyanine Green Fluorescence Imaging Navigated with Preoperative CT Lymphography for Superficial Esophageal Cancer, Ann Surg Oncol (2012) 19: 486 – 493
Q&A
Thank you
Quantitative evaluation
Method ICG emits light with a peak wavelength of 830 nm when illuminated with near-infrared light Blood flow in the gastric tube was recorded by a Hyper Eye Medical System (HEMS, Mizuho Corporation) Continuously recorded the data for 5 minutes
Method Quantitative assessments of perfusion at 2 places in the gastric tube (Point A, the last branch of the right GEA; Point B, 3 cm proximal to Point A
Method Y = luminance Blood perfusion determined by pattern of luminance change
Result
Result
Conclusion? ICG fluorescence angiography may be used quantitatively to measure blood perfusion of the reconstructed gastric tube in patients undergoing esophagectomy.
Limitation Number of patients way too small Unable to confirm any association between blood flow type and clinical outcomes (leakage) The location of the anastomoses in the gastric tube differed among patients Patients’ anatomy were variously biased