JOB VAN WOENSEL KINDERARTS INTENSIVIST AMSTERDAM UMC J

JOB VAN WOENSEL, KINDERARTS INTENSIVIST AMSTERDAM UMC J. B. VANWOENSEL@AMSTERDAMUMC. NL CIRCULATORY SUFFICIENCY IN RESOURCE POOR

UNDER 5 MORTALITY

UNDER 5 MORTALITY
")
IN-PATIENT CHILDHOOD MORTALITY IN RPS ▸ 65% in the first 24 h (Menge 1995) ▸ ‘mostly’ in the first 48 h ▸ 33% in the first 48 h (Ahmed 1999) (Maitland 2006)

IN-PATIENT CHILDHOOD MORTALITY IN RPS 100 80 60 % 40 20 0 0 2 4 6 8 10 12 14 16 18 20 Day of admission 22 24 26 28 30 32 34
 ▸ Septic shock:")
CIRCULATORY INSUFFICIENCY IN RPS ▸ Overall mortality: 21% (CI 16 -26%) ▸ Septic shock: 33% (CI 24 -43%) ▸ Gaps: - Lack of uniformity in definitions! - Difficult to define pathophysiology (guide to Rx)

GOALS OF SHOCK TREATMENT ▸ recognition…. ▸ first line treatment….

CIRCULATORY INSUFFICIENCY: CURRENT GUIDELINES

FIRST LINE TREATMENT SHOCK, INTERNATIONAL GUIDELINES ‣ Intravenous fluid with 20 ml/kg crystalloids in 15 min ‣ Repeat up to total of 60 ml/kg ‣ Guided by restoration of circulation (Davis 2017)

FEAST TRIAL: DESIGN ‣ Patients: - children with severe febrile illness with impaired perfusion complicated by impaired consciousness a/o respiratory distress ‣ Intervention: - 20 ml/kg bolus fluid (normal saline or albumin) ‣ Controls - Maintenance of fluids ‣ Endpoint: - mortality at 48 hours

FEAST TRIAL: RESULTS • Mortality at 48 h: - 110/1047 children in the saline-bolus group (10. 5%) - 111/1050 children in the albumin-bolus group (10. 6%) - 76/1044 children in the control group (7. 3%) • Relative risk of death - fluid bolus vs no bolus: 1. 45 (P=0. 003) • Post hoc analysis: - Cardiovascular collapse contributed to over-mortality

SHORT TERM CONSEQUENCES FEAST TRIAL ‣ Discrimination in type of shock is important ‣ Be reserved with iv fluids in patients with septic shock ‣ Give iv fluid in hypovolaemic shock! - e. g. In case of diarrhoea, blood loss


OXYGEN SUPPLY ▸ Arterial oxygen content ▸ Cardiac output ▸ Oxygen delivery ▸ Oxygen extraction

Cardiac Malnutrition CAUSES Severe infection Diarrhoea Viral infection Malaria Anemia Trauma SYNDROME: SHOCK DISTRIBUTIV HYPOVOLAE E MIC TREATMENT OBSTRUCTI VE DISSOCIATI VE CARDIOGEN IC TREATMENT TREATMENT

CIRCULATORY INSUFFICIENCY IN SUBSAHARAN AFRICAN CHILDREN CISSAC STUDY ▸ Aims - Investigate etiology of shock - Classify pathophysiology of shock ‣ Secondary aims - Define discriminative predictors - Investigate practical and simple interventions - Predict fluid responsiveness


 ▸ Extensive investigation")
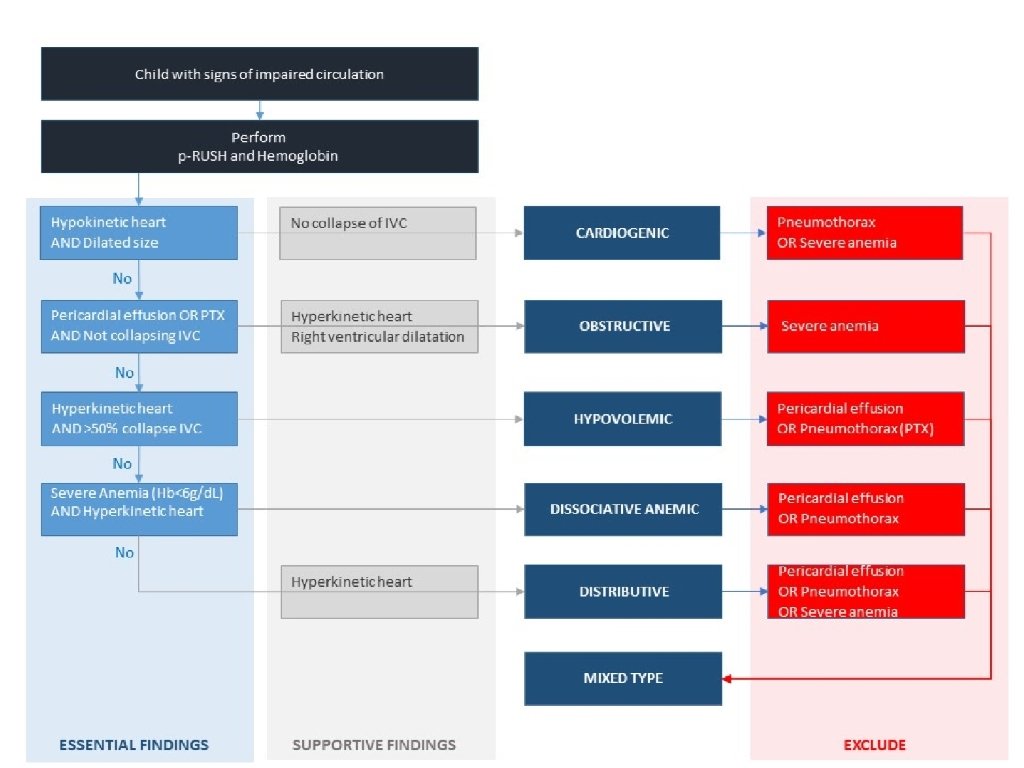
PILOT STUDY ▸ 40 children with circulatory insufficiency (definition FEAST trial) ▸ Extensive investigation of etiology ▸ Classification of the pathophysiology based on: - clinical signs - vital signs - laboratory investigations - cardiac ultra sound
 ▸ Extensive investigation")
PILOT STUDY ▸ 40 children with circulatory insufficiency (definition FEAST trial) ▸ Extensive investigation of etiology ▸ Classification of the pathophysiology based on: - clinical signs - vital signs - laboratory investigations - cardiac ultra sound - innovative non-invasive tools

Compensatory reserve index Heart rate variability

Sidestream dark field imaging

CONCLUSION ▸ Under 5 mortality in RPS: still a major problem ▸ In-hospital mortality shock in RPS: high in first days! ▸ FEAST trial: controversy about iv fluid ▸ IV fluid: not ‘one size fits all’ ▸ Difficult to discriminate pathophysiology of shock ▸ Research is needed

- Slides: 29