JHSGR Management of blunt splenic injuries Dr PT

JHSGR Management of blunt splenic injuries Dr PT Chan /QEH

Introduction Spleen is the most frequently injured organ in blunt trauma n Spleen plays an important role in immune function n n Overwhelming Post splenectomy Infection (OPSI) 0. 05 -2% n Mortality 50%-70% Takehiro Okabayashi, . World Journal of Gastroenterology 2008

n Change in the approach to splenic injury n Operative splenic preservation achieved by splenorrhaphy has progressed to the nonoperative management.

Etiology and Risks n Trauma n Rapid deceleration n n Road Traffic Accidents Direct force n Fell from height/ sports n Iatrogenic n Risks: Pre-existing illness n Splenomegaly due to haematological disease / malaria/ Infectious mononucleosis

Clinical presentation Left upper quadrant abdominal pain n Left shoulder tenderness (referred pain from subdiaphragmatic nerve root irritation) n Peritoneal sign n Signs and symptoms of shock n e. g. tachycardia, restlessness, tachypnea

Investigation n USG n FAST : Look for any free peritoneal fluid n Sensitivity n Splenic injuries n n 55%-91%, specificity 97 -100% sensitivity 41 -63%, specificity 99% CT scan n Splenic injuries n Sensitivity 95% , specificity 100%

AAST Grading of splenic injury

Grade 1 n n Subcapsular hematoma of less than 10% of surface area. Capsular tear of less than 1 cm in depth.

Grade 2 n n n Subcapsular hematoma 10 -50% of surface area Intraparenchyml hematoma < 5 cm diameter Laceration of 1 -3 cm in depth and not involving trabecular vessels

Grade 3 n n Subcapsular >50% surface area or expanding Ruptured subcapsular or intraparenchymal hematoma Intraparenchymal haematoma >5 cm or expanding Laceration of greater than 3 cm in depth or involving trabecular vessels

Grade 4 n Laceration involving segmental or hilar vessels producing major devascularization (>25% of spleen)

Grade 5 n Shattered spleen / Hilar vascular injury

Management

Haemodynamic unstable n Surgical intervention Laparotomy n 4 quadrants packed n Assess the extent of splenic injuries n n Only if feasible, may consider conserving the spleen n Otherwise, Splenectomy should be performed Excluded other injuries n Splenorrhaphy n n Parenchymal suture/Fibrin glue/ABC/ Laser/omental patch/mesh bag/partial splenectomy

Haemodynamic stable n Non operative management with close monitoring n n Vital signs, haemoglobin levels Successful rate 80% ~89. 2% Jason Smith. Journal of Trauma 2007 Andrew B. Peitzman, . Journal of Trauma 2000.
 occur within")
Non operative management n How long should be monitored? most failure( 95%) occur within 3 days(72 hrs) of admission. (97% in 5 days, 99 % in 30 days) n Suggested patients to be closely monitored for 3 -5 days n Highly dependency unit and step down Jason Smith. Journal of Trauma 2007 afterwards n

Successful rate of NOM Jason Smith. Journal of Trauma 2007

Non operative management n Risk factors for failure Higher grading of splenic injuries n larger quantity of haemoperitoneum n older age n Contrast extravasations in CT n Jason Smith. Journal of Trauma 2007 Siriratsivawong K Am Surg 2007 Andrew B. Peitzman. Journal of Trauma 2000.

Non operative management

Andrew B. Peitzman. Journal of Trauma 2000.

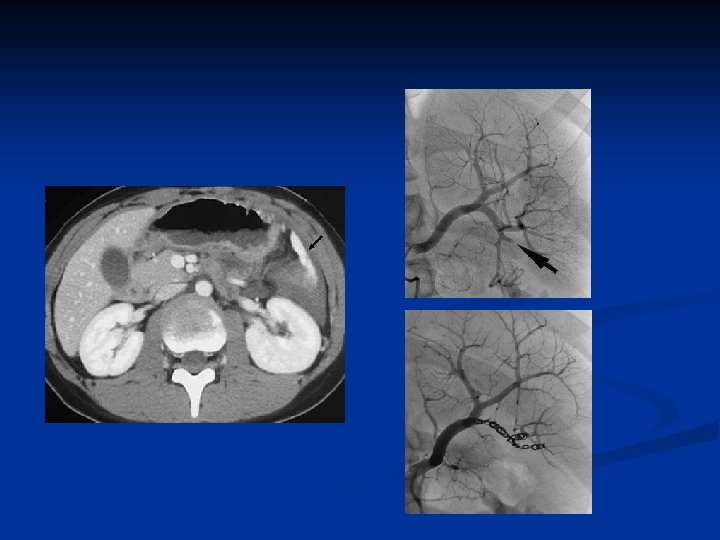
Angioembolization n Increased successful rate of non-operative management in selected policy n n Increase up to 97% Indications: n Contrast extravasation, pseudoaneurysm, grade 4 injuries Ashraf A. Journal of Trauma 2009
, rebleeding (19%), splenic atrophy (4.")
Complications of embolization n Total splenic infarction (9. 5%), rebleeding (19%), splenic atrophy (4. 8%), partial infarction (38%), pleural effusion (33%). Shih-chi Wu. World journal of surgery 2008

Resolution and Progression n Time of mobilization? No definite guidelines, earlier for low grade injuries. n 77% mobilization within 72 hrs after admission n Day of mobilization was not associated with delayed splenic rupture. n London JA. Arch Surg. 2008.
 Stephanie A. Journal of Trauma. 2008")
% of patients remained unhealed over time (days) Stephanie A. Journal of Trauma. 2008

Activity Restriction-Athletes n No consensus on return to play after splenic injury n Acceptable to engage in light activity for the first 3 months and then gradually return to full activity Elizabeth H. American College of Sports Medicine. 2010.

Follow up No evidence that routine follow up serial CT scans without clinical indications influenced the outcome or management. n Imaging maybe considered if patient has a high grade of injury/ still experiencing symptoms n Thaemert BC. Journal of Trauma 1997

Prevention of Infection n Vaccination Pneumococcal , then booster after 5 years n Hamemophilus influenza B n Meningococcal every 3 -5 years n Two weeks after emergency splenectomy n Education n Bracelet/Card n Guidelines from the Centers for Disease Control and Prevention Shatz DV. Journal of trauma 2002, 1998

n Antibiotic prophylaxis No clinical trials in adults n “Standby” antibiotics n Some suggest 2 -5 years prophylaxis n Long term prophylaxis not generally recommended n DC. The Netherlands Journal of Medicine 2004

Summary n n n Operation if haemodynamic unstable Only stable patient are admitted for observation for 3 -5 days CT for assessing degree of injuries n n n Grade 5 injuries need operation Majority of grade 4 splenic injuries are unstable and likely need to be operated Angio/embolization can be considered for stable patients with contrast extravasation or pseudoaneurysm Advise activity restriction according to the grade of injuries Vaccination /education for infection prophylaxis Follow up CT scan should be considered in selected patients

Management

Thank You
 Computed")
n Latent pseudoaneurysm may present ~ 24 -48 hrs after injury (2. 2%) Computed Tomography Identification of Latent Pseudoaneurysm after blunt splenic injury : Pathology or Technology

Hunter B. Long-Term Follow up of Children with nonoperative management of blunt spenic trauma. Journal of Trauma 2010.

Splenorraphy Grade 1: haemostatic agent Grade 2 : 43% + suture/mesh Grade 3 : 100% + suturing /parenchymal suture Grade 4: anatomical resection Grade 5: splenectomy Pickhardt. B, Operative splenic salvage in adults: a decade perspectives. Journal of Trauma 1989

Paediatric patients n Mechanism of injury: n n n Complications n n More fall or sports than RTA Elastic ribs readily change contour and cause rapid flexion of organs along its axis -> lacertions are more oriented to the larger segmental vessels Thicker and more fibrous splenic capsule Tolerate higher grade of injuries with non operative management Very low incidence For delayed splenic rupture (0 case in one metaanalysis 1083 patient vs 5 -6% in adult) Most pseudoaneurysm will spontaneously resolve or self tamponade Non-operative management is the standard for all grades of splenic injuries in all haemodynamic stable patients (75 -93% successful rate) Peditric blunt splenic trauma: a comprehensive review Pediatr Radiol (2009)39: 904 -916

Andrew B. Peitzman, Blunt Splenic Injury in Adults: Multiinstitutional Study of the Eastern Association for the surgery of Trauma. Journal of Trauma 2000.

Activity Restriction n Light activity n n Strenuous activity n n Light housework, office work, low impact aerobic activity Running, lifting over twenty pounds, cosntruction work, manual labor Full activity (contact sport)

Fata P. A survey of EAST member practices in blunt splenic injury; a description of current trends and opportunities for improvement. Journal of Trauma 2005

Late complication of splenic injuries n Non operative Delayed rupture spleen 1% n Splenic Pseudocyst n Splenic necrosis/abscess n n Splenectomy n Overwhelming postsplenectomy Infection (OPSI)
- Slides: 40