IVUS Guidance for CTO Mehrdad Taherioun MD Fellowship




































- Slides: 38
IVUS Guidance for CTO Mehrdad Taherioun MD Fellowship of interventional cardiology Modarres hospital
Ultrasound Principles
Forward-Looking IVUS Under FL-IVUS guidance, the wire is advanced into the true lumen
IVUS IMAGE
Functions of IVUS • • • Makes Sure Vessel Size and Character Decides Stent Size and Position Evaluates Stent Expansion and Apposition Evaluates Dissection at Stent Edge Finds Entry of CTO
CTO‐PCI:current approach Satoru Sumitsuji MD FACC
Antegrade technique
IVUS for wiring an Abrupt Type CTO • Blunt stump with the presence of side branch • Side branch large enough to accommodate the IVUS catheter
Blunt stump with the presence of side branch
Baseline bilateral coronary angiography showing possible entry points
Identify a CTO entry by IVUS • Pull back and push forward with the IVUS catheter around the proximal cap • Keep the IVUS transducer in that position • Using a stiffer wire, or even tapered tip wire, advance the wire tip to the proper location • Torque the wire in the right direction and make several quick pushes with the wire to penetrate the lesion
IVUS transducer at the optimal entry point
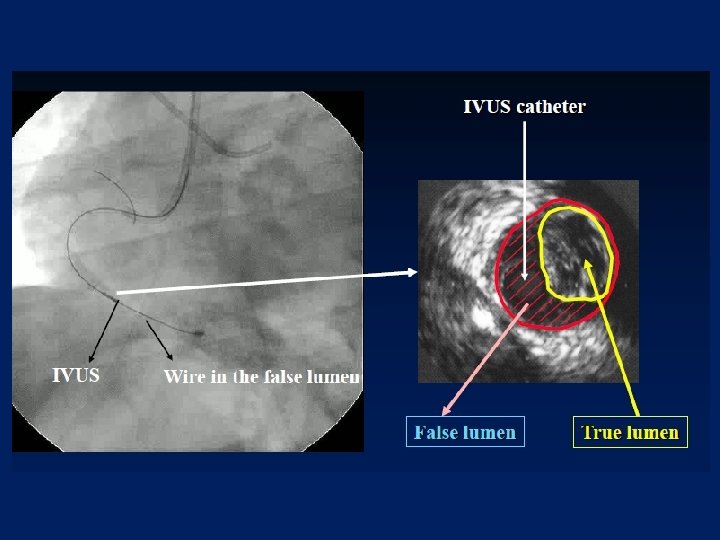
Identify a CTO entry by IVUS • Sometimes, parallel wiring technique is useful in this situation • However, the guide-wire may still enter the false lumen
Wire in Sub?
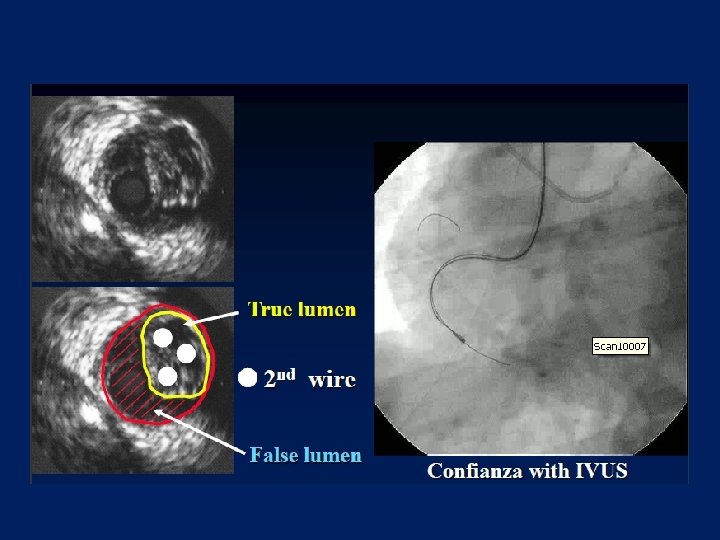
Wire in True!
IVUS guided Reentry technique Step 1: making system for IVUS guided reentry Step 2: dilating lumen for advancing IVUS Step 3: assess and decide strategy Step 4: wiring to get distal true lumen Satoru Sumitsuji MD FACC
Step 1: making system for IVUS guided reentry • GC ≥ 7 Fr or double GC ≤ 6 Fr Advance both IVUS cath and CTO wire with microcatheter
Step 2: dilating lumen for advancing IVUS 1. 5 or 2. 0 mm balloon angioplasty
Step 3: assess and decide strategy • Identify subintimal tracking segment • Reentry point location and direction • Plaque characteristics; calcification
Step 4: wiring to get distal true lumen • Repeat wiring followed by IVUS check until wire get plaque or true lumen • Wire type: usually stiff wire is required
Failure to cross
IVUS guide re-entry of wire
Reentry point location and direction
IVUS in Retrograde approach Reverse CART Technique
Functions of IVUS in retrograde approach • Makes Sure Retrograde Wire Position • Decides Balloon Size for R-CART • Knows Appropriate Site for R-CART
Typical subintimal & intimal image
IVUS Inside CTO
IVUS Findings
Both Wires in Intima Reverse CART Toyohashi Heart Center
Both Wires in Sub-Intima Toyohashi Heart Center
Antegrade Wire in Intima Retrograde Wire in Sub-Intima Toyohashi Heart Center
Antegrade Wire in Sub-Intima Retrograde Wire in Intima Toyohashi Heart Center
Antegrade Wire in Sub-Intima Retrograde Wire in Intima
Penetration Using Confienza Pro 12
summary 1. In an antegrade approach, IVUS could identify entry of CTO located at bifurcation. 2. In a retrograde approach, we could know position of retrograde wire and appropriate balloon size for RCART. 3. IVUS could resolve problems when R-CART dose not work well.
Thank you for your attention