IV Therapy Starting IV infusions IV medications Administration



: 70 -110” long, 20 -30 ml to prime –")


 most used for infusions �Larger the number,")













 �Name/date/time")



- Slides: 25
IV Therapy Starting IV infusions & IV medications Administration,
Osmolality • Reflects Concentration of a solution • Normal serum m. Osm/L generally 290 -300 – Fluid stays where infused – Useful for hypotension, stays in vessels • Hypertonic: post operative often – Reduces risk of edema, stabilizes BP & regulates urine output • Hypotonic: fluid shift into cells – Hyperglycemia, HHNKS, over diuresis – Don’t use for IICP or cerebral edema
Intravenous Fluids: Crystalloids • Isotonic: IV fluids from 275 -295 m. Osm/l – D 5%W, 0. 9% NS, Lactated Ringers – Increases extracellular/intravascular volume • Hypotonic: less than 275 m. Osm/l – D 2. 5%W, 0. 45% NS, 0. 33% NS – Lowers osmotic pressure of plasma so fluid enters cell • Hypertonic: greater than 295 m. Osm/l – – D 5% in 0. 45 NS, D 5% in 0. 9% NS D 5% in Lactated Ringers 10% Dextrose or 3% Sodium Chloride Increases osmotic pressure to draw fluid from cells into vascular
Administration Sets • Basic (Primary): 70 -110” long, 20 -30 ml to prime – Often have backcheck valves, Y sites • • • Add-on (secondary): 7 -10 ml to prime Microdrip: 60 drops/minute Macrodrip: 10, 15 or 20 drops/minute These are your drop factors Must hang at least 36 inches above site
Filters • Add on or in-line, distal in tubing, close to patient • Remove pathogens, particles & air • Decreases risk of infection/phlebitis • 0. 2 micron most common • Follow manufacturer & facility protocols for priming & use
IV Start Steps and Considerations
IV Cath Selection �Catheters: Over-the-needle catheter (ONC) most used for infusions �Larger the number, smaller gauge of lumen ◦ 16 gauge is large bore, 24 gauge is small bore ◦ gauge should be smaller than vein lumen �Needle shields incorporated in newer designs �Needleless connection systems
Site Prep • Clip hair if necessary, shaving causes micro-abrasions which can cause infection • Towel or disposable pad under site • Skin prep with antiseptic, allow 30 seconds to dry, or pat dry with gauze, will be using chloraprep • Prepare tape strips, flushing of extension • Apply gloves if not already on • No popping out a finger!!
Chloraprep • Simply pinch the wings on the applicator to pop the ampule. • Hold the applicator down to allow the solution to saturate the pad. • To maintain the asepsis, it is important not to touch the pad. • Press sponge against skin & apply using back & forth friction for 30 sec & allow to dry • Discard applicator after single use �Chlora. Prep-1. 5 m. L-Frepp- Applicator. aspx
Connecting Tubing • Release tourniquet • Exert pressure above end of needle/cannula in vein to occlude venous return • Remove introducer, use safety feature, connect primed plug, extension set with flush or tubing • Aspirate and flush or allow solution to flow – Check for swelling, slow flow – If hematoma develops, remove/ apply pressure
IV Securement • Place occlusive dressing over insertion site – transparent semipermeable membrane (tegaderm, op-site) 72 -96 hrs per CDC – if gauze used, change in 48 hrs – DO NOT pull tight- will itch • Tape per facility guidelines • Label with type, size, date, time, initials
Maintenance • • Stat-Lock catheter securement devices Stretch net dressing Range of motion test of flexion/extension Armboard if near joint, check frequently – Can cause nerve & tendon damage – Provide ROM • Document initiation of IV catheter • Document maintenance per hospital policy • Pt Education as described earlier
Changing IV Site and Dressing • Ideally done at same time • Usually 72 hrs, up to 96 if dressings intact • Sterile gloves if changing down to cath hub • Sterile gauze under cath hub • Many use short extension sets & caps that maintain catheter sterility & facilitate tubing changes • Follow facility protocols • Document site, dressing, tubing changes
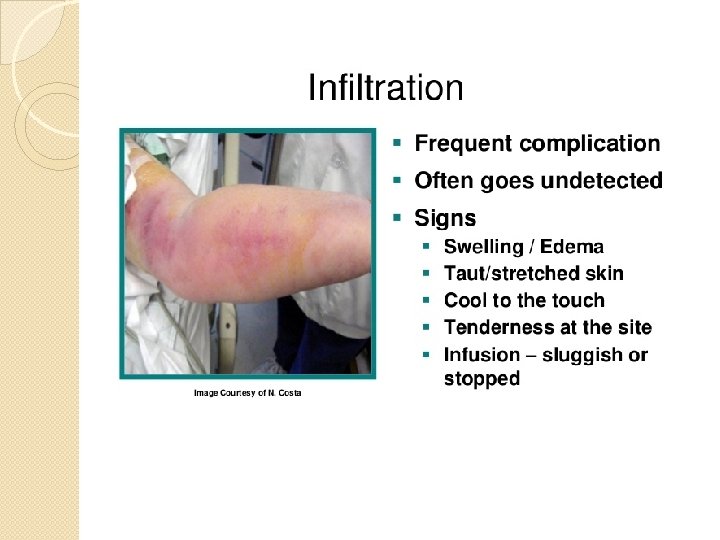
Complications • • • Phlebitis Infiltration Catheter Dislodgement Occlusion Vein irritation/pain Severed catheter Hematoma Venous spasm Thrombosis Thrombophlebitis Nerve, tendon, ligament damage
Infiltration • Infiltration: Dislodgement of cannula with leaking of fluid into surrounding tissues • Risk increases when near joint – Blanching of site, lack of blood return – edema deprives patient of fluid and drug – limits available veins, predisposes to infection • To confirm, apply tourniquet to block venous flow – If infusion continues , infiltration has occurred – Remove cannula – Warm soaks to aid absorption, Elevation of limb
Phlebitis • Erythema & pain – Tenderness at cath tip, elevated temp – Painful redness along the length of vein. – Puffy area over vein, Hard on palpation • Potential for embolism if clot breaks off of wall • Caused by friction, poor blood flow, irritation from medications • Remove catheter & apply warm soaks, elevate • Vein irritation from solution with low or hi p. H or osmolarity: KCl, Dilantin, Valium, Vancomycin
Extravisation
Documentation • Evidence that prescribed treatment given • Record for health care insurers of equipment & supplies used. • Progress notes, flowsheets • Medication/IV record • Intake/Output records
Initial IV Placement Documentation �Size, length, type of �Number of attempts catheter (successful/unsuccessful) �Name/date/time of catheter insertion �Site location (vein name preferred) �Type of solution/additives � Flow rate/use of infusion device/rate control �Complications/patient response/nursing interventions �Pt education & evidence of understanding
IV Maintenance Documentation �Condition of site/site care provided �Dressing changes �Solution/tubing changes �Teaching & evidence of understanding �Intake & Output: Record all IV intake o Infusions, flushes, medications, blood, TPN o Total balances q shift o Hourly outputs if critical care
IV D/C Documentation �Validate order to discontinue &/or note reason for discontinue � Time/Date /amount of fluid infused �Assessment of site before & after access device removed �Complications/pt reactions/ nursing interventions �Integrity of venous access device at removal, tip intact? �Follow-up actions (IV restart? ) �IV Start
Credits � Donna Elmore RN-BC, CNRN, BSN, MS �Donna Wheeler MSN, RN �IV Therapy made Incredibly Easy, 4 th Edition, 2009