IT AINT WHAT YOU DO ITS THE WAY










 Such as a physical health problem, retirement, bereavement etc.")
 Life event leads to fewer behaviours that provide value and meaning")
 …which leads the person to feel low")
 Attempts to cope may include avoidance behaviours, which can maintain the")
 Avoidance behaviours are negatively reinforced Reduction in positive reinforcement")





: 611 -623.")
 Effect size -0.")



")






 to CBT (gold standard)")

 Mean (95% CI) 219")

 CBT N Baseline BA Mean (SD) 219")












 Collaborative")




























- Slides: 81
IT AINT WHAT YOU DO IT’S THE WAY THAT YOU DO IT. USING BEHAVIOURAL ACTIVATION AS A PSYCHOLOGICAL INTERVENTION TO TREAT AND PREVENT DEPRESSION (IN THE THIRD AGE) Professor David Ekers Ph. D, MSc ENB 650, RMN
The talk What is BA/how does it work The evidence for BA to treat depression-a pragmatic choice Can it prevent depression (the CASPER study) Current ongoing studies
The intervention Behavioural Activation
Background to BA Skinner 1950’s introduces the operant conditioning. Observes depression associated with a break from established sources of positive reinforcement from environment Ferster 1973 -When stable sources of positive reinforcement lostdepression occurs-activity scheduling treatments introduced Showed promise in early randomised controlled trials Until the cognitive model took over in 1980 s External to the person Views depression as an understandable response in the context of client’s lives. Looks at depression as a consequence of person-environment interactions As such this relationship ‘person-environment’ is focus of the treatment
But may be somewhat older!
Robert Burton 1626 ‘I write of melancholy by being busy to avoid melancholy’ Connection between the mind and the body Emphasised the ‘creative blessings’ which come with melancholy Proposed activity, creativity and interaction with the natural world as a treatment
A reminder of Behavioural principles of reinforcement
Reinforcement Presented Positive Negative Omitted Positive Reinforcement Frustrative non reward Punishment Negative Reinforcement
Practical daily use of negative reinforcement
Behavioural activation cycle rationale (developed for our 2011 study
Behavioural activation (BA) Such as a physical health problem, retirement, bereavement etc.
Behavioural activation (BA) Life event leads to fewer behaviours that provide value and meaning in life
Behavioural activation (BA) …which leads the person to feel low
Behavioural activation (BA) Attempts to cope may include avoidance behaviours, which can maintain the problem
Behavioural activation (BA) Avoidance behaviours are negatively reinforced Reduction in positive reinforcement
Life event Became ill with diabetes and heart problems Secondary problems, friends stopping coming round Coping by avoidance: When friends called George didn’t feel up to going out so would make excuses. He stopped going to allotment even for short periods and hardly ever saw his friends Behavioural activation worked here to stop the cycle going round and worsening. Through step by step activity George gradually started to be more active towards his goals and broke the cycle. Isolation from valued activities: This led to not being able to do as much at the allotment and not going to football. George also had to reduce alcohol so didn't see friends as much Feeling Bad: Gradually George felt his confidence drop and he felt tired all the time. Some of this was illness and some low mood. He had no motivation to do any more than watch TV
BA Key Principles Relies on sound therapeutic alliance and collaborative relationship Focus on meaningful connection with the world ‘Outside-In’ rather than ‘Inside-Out’ approach � We don’t tell people to wait for some internal state to change before they can begin to change. � Change the outside and the inside will change � Rather than ‘waiting to feel better to do it’ – ‘do it to feel better’
R 2 D 2’s BA guide to treating depression Two Rs: Re-instate previous behaviours Replace old behaviours with new Two Ds: Disrupt unhelpful patterns of behaviour Decrease avoidance behaviours
Valued goals/not just any activity-need good targeting- Case examples scheduling for emotional goals
BA and depression
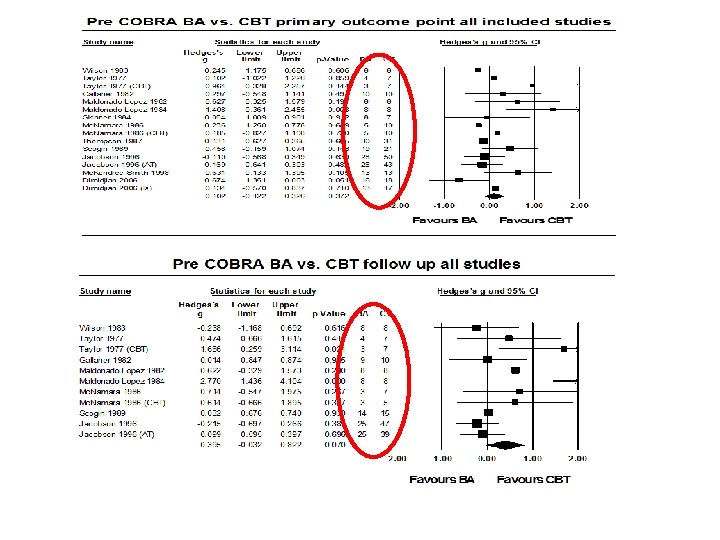
A long-long time ago Psychological Medicine 2008; 38(5): 611 -623.
Findings in 2008 BA vs. Control/Usual Care 12 studies (459 participants) Effect size -0. 70 in favour of BA (large) (95% CI − 0. 39 to − 1, p=0. 001), recovery rate favours BA OR= 4. 18 CI 1. 14 to 15. 28 (p=0. 03) BA vs. CT/CBT Twelve studies (476 patients) No difference effect size at post treatment and follow up (SMD 0. 08 95% CI − 0. 14 to 0. 30, SMD of 0. 25, 95% CI − 0. 21 to 0. 70, p=0. 28) or recovery rate (OR 0. 92, 95% CI 0. 59 to 1. 44, p=0. 72)
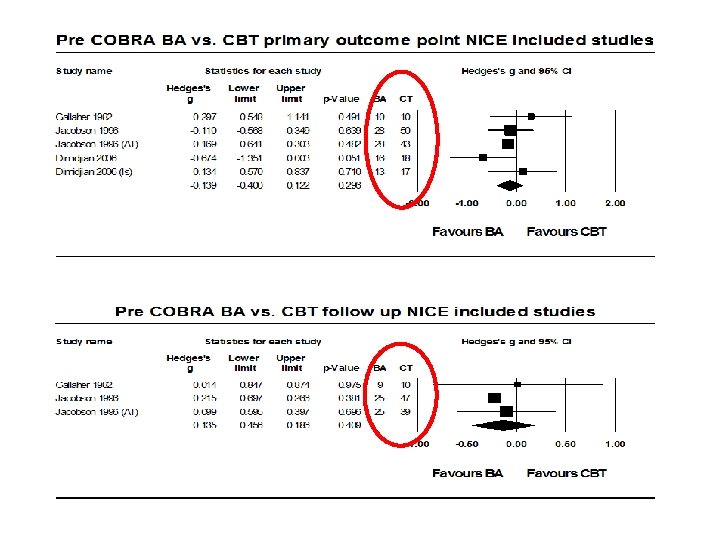
When you take out the dodgy ones
Evidence gap in 2008/9 All studies used highly qualified therapists Small studies of questionable quality NICE (2009) made a clear research recommendation “to establish whether behavioural activation is an effective alternative to CBT” using a study “large enough to determine the presence or absence of clinically important effects using a noninferiority design”
First step- test the feasibility of the idea of non specialist delivery
Results at follow up (3 months post randomisation n=47)
Economic Analysis Ekers D, Godfrey C, Gilbody S, Parrott S, Richards D, Hammond D and Hayes A. (In Press BJ Psych)
Cost more/less effective Cost less/less effective Cost more/more effective Cost less/more effective
Beware
Small Study - Big Limitations Small sample 2 therapists No follow up Strong signs of proof of principle and used as basis for COBRA and CASPER study applications
Open access- The Lancet July 2016
COBRA is a two-arm Phase III, non-inferiority randomised controlled trial of a psychological intervention: Behavioural Activation (BA) N=440. The COBRA programme of research sought to answer two interlinked questions: � What is the clinical effectiveness of BA (non specialist) compared to CBT for depressed adults in terms of depression treatment response measured by the PHQ 9 at six, 12 and 18 months? � What is the cost-effectiveness of BA compared to CBT at 18 months?
COBRA Hypotheses BA is non-inferior (1. 92 PHQ 9 points) to CBT (gold standard) for depressed adults in terms of depression treatment response at twelve and 18 months BA is more cost-effective than CBT at 18 months
What we found
CBT Baseline BA Adjusted A-B difference* P-value N Mean (SD) Mean (95% CI) 219 17. 4 (4. 8) 221 17. 7 (4. 8) - - 189 8. 4 (7. 5) 175 8. 4 (7. 0) 0. 1 (-1. 3 to 1. 5) 0. 89 151 7. 9 (7. 3) 135 7. 8 (6. 5) 0. 0 (-1. 5 to 1. 6) 0. 99 Intention to treat 12 -months Per protocol 12 -months *Adjusted for baseline PHQ 9, and stratification variables (i. e. , symptom severity (PHQ < 19, PHQ ≥ 19), site (Devon, Durham, Leeds), antidepressant use (currently taking anti-depressant medication, not currently taking antidepression medication)
Non inferiority margin Non-Inferiority at primary endpoint
Secondary Outcomes – What about anxiety (GAD-7) CBT N Baseline BA Mean (SD) 219 12. 6 (5. 1) Adjusted difference* P-value N Mean (SD) Mean (95% CI) 221 12. 7 (5. 1) - - 161 6. 4 (5. 9) 0. 1 (1. 3 to -1. 0) 0. 82 129 5. 9 (5. 5) 0. 01 (-1. 3 to 1. 2) 0. 95 Intention to treat 12 -months 176 6. 3 (6. 0) Per protocol 12 -months 146 6. 0 (5. 8) *Adjusted for baseline GAD, and stratification variables (i. e. , symptom severity (PHQ < 19, PHQ ≥ 19), site (Devon, Durham, Leeds), antidepressant use (currently taking antidepressant medication, not currently taking anti-depression medication)
ECONOMICS
Cost Effectiveness Plane Cost More/More Effective Cost More/Less Effective Difference in cost 6% £ 500 4% -. 05 0 . 05 . 15 -£ 1000 -£ 500 -. 1 £ 0 Difference in QALY 24% Cost Less/Less Effective £ 20 k/QALY threshold line 66% Cost Less/More Effective 95% confidence ellipse
Clinical Implications BA delivered by less experienced mental health workers leads to identical clinical outcomes for patients with depression, but at a financial saving to clinical providers of 21% compared with the costs of providing CBT. This is particularly relevant to the dissemination of effective psychological interventions for depression globally, particularly in low and medium income countries.
Using BA to prevent depression
Rationale-BA to Prevent Depression in over 65 s Can be delivered by non specialists Possibly a good public health message Makes sense to people
The CASPER trial Collaborative Care for Screen Positive Elders
CASPER Care for Screen Positive Elders
CASPER Care for Screen Positive Elders
CASPER Care for Screen Positive Elders
Who took part? 705 participants Over 65 s – mean age 77 (range 65 – 99 yrs) Whooley +ve with DSM-IV Subthreshold depression Very few exclusions � Recently bereaved � Alcohol dependence � Terminal illness � Cognitive impairment (ascertained by the GP) Comorbidity OK – 80% or more had 2+ LTCs
Collaborative care Case manage r Primary care physicia n Older adult Mental health speciali st Non-specialist Liaises with other health professionals Symptom monitoring Brief psychological treatment Over the phone Medication management
Functional equivalence Life events as we get older � � Physical health conditions Bereavement Retirement Change / loss of roles } These life events may make it difficult or impossible to reinstate previous behaviours Functional equivalence � � � Behaviours may look very different but serve the same function What function did the previous behaviour serve? Are there different behaviours that may serve the same function?
Design Recruitment from primary care Older adults with sub-threshold depression (N = 705) Collaborative care (with BA) (n = 344) Treatment as usual (N = 361) PHQ-9, GAD-7, PHQ-15, EQ-5 D, SF-12 (4 and 12 months)
er th 40% O n tio nd i co 11% e er an c 14% Ey C is rit th ar eo st is rit th ar 9% O d is os po r eo oi at um he R st es iti on nd co be t ia ro ke 20% O ry to ra pi es St e as se di 8% D rt ea re su es pr ol 6% H od bl o oh 50% R h ig Al c er 10% H ok Sm Physical health problems in CASPER 60% 48% 30% 30% 25% 21% 22% 17% 12% 0%
Outcomes @ 4 and 12 months PHQ 9 – continuous measure and ‘caseness’ for depressive disorder SF 12 GAD 7 PHQ 15 RISC 2
ar M 11 ay -1 Ju 1 l-1 Se 1 p. N 11 ov -1 Ja 1 n. M 12 ar M 12 ay -1 Ju 2 l-1 Se 2 p. N 12 ov -1 Ja 2 n. M 13 ar M 13 ay -1 Ju 3 l-1 3 M CASPER trial recruitment 800 700 600 500 400 200 100 0 target consented 300 actual consented
Primary outcome
PHQ 9 scores at 4 and 12 months
Does collaborative care prevent the onset of depression?
Did collaborative care prevent case level depression? Odds of case level depression were halved at 12 months OR = 1. 98 (1. 21 to 3. 25)
Did collaborative care prevent case level depression? Odds of case level depression were halved at 12 months OR = 1. 98 (1. 21 to 3. 25)
Is there a preventative element to CC? Odds of case level depression were halved at 12 months OR = 1. 98 (1. 21 to 3. 25)
What about secondary outcomes? SF 12 GAD 7 PHQ 15
SF 12 physical component score
SF 12 mental component score
GAD 7
PHQ 15 – somatoform complaints Symptoms for which the greatest improvements were observed were: Pain in arms, legs or joints; Dizziness; Shortness of breath; Constipation, loose bowels or diarrhoea; and Trouble sleeping.
What about antidepressants?
Some qualitative findings
BA and collaborative care Cos I suppose that the ideas are very kind of common sense but perhaps it’s this going through a more kind of formal process of like analysing what you do, how you feel, how they relate to each other and then sort of writing things down, I guess people say that’s helpful to …reflect and then think about what they might like to change…. . little things.
Functional equivalence But I think it was very good later on in the thing [booklet] where it said, ‘What could you do to replace, erm, you know, various activities if you had to stop doing them’. And I think that was good, to help you think round things
Using the phone Because I don’t like talking on the telephone all that much because of sort of interviews where you try and sort something out like your telephone or your inter, internet or something, and people talk too fast and too quickly and you feel terribly slow, but she wasn’t like that at all. She was very clear and patient … and it was fine, and relaxed and yeah. I thought it would be odd talking over a telephone about yourself, but it was alright.
Phone vs face to face Int: So would you have preferred having it face to face, all the sessions face to face? Q 11347 F: Well I think, yes I mean one would say that, but it wouldn’t matter. It’s, erm, …. it’s slightly self-indulgent having face to face [interactions] I think
And the cash!
Was it cost effective? Direct costs of collaborative care = £ 494 Some evidence of cost offset - £ 55 Worst case cost/QALY £ 9, 633 CC as delivered cost/QALY £ 3328
Was it cost effective?
Summary of findings Good engagement; liked the BA focus of the intervention and telephone management Moderate effect size 0. 3 Positive across a range of outcomes (signs in Physical and psychological functioning) Prevented the onset of case level depression (based on PHQ scores) Cost effective Largest UK trial of collaborative care to date Largest ever trial of CC for subthreshold depression
Our Current studies/collaborations Community Pharmacy Mood Intervention Study CHEMIST- Feasibility and Pilot study- Intervention adaption and Pilot RCT-results due early 2020. Good engagement and signs can deliver in innovative new settings- ave age 65 Multi-Morbidity in Older Adults (MODS)- 6 year program grant for applied research-adaption of BA to target functioning in over 65 s with 2 or more LTC inc depression. 3 or more LTC in people over 65 with sub threshold up to major depression-flexible BA design to target functioning
BA collaborations Impact BEACON study. Adaption of BA in South Asia settings with co morbid non Communicable disease. Insika Yomama. BA delivered by community workers in South Africa in perinatal depression with HIV+ status. Ba. NDep. BA for depression in Elderly care homes in Melbourne and Perth Depression prevention in older adults in Brazil using BA focused targeted health promotion audio messages. Audio whats app!-Sao Paulo-BA advice and case stories via audio message-story arc over 4 themes and upp to 48 1 minute messages.
Summary BA is a practical treatment aiming to re engage people with positive reinforcement from their environment. Evidence in adults-older adults suggest it works well Evidence in younger people is limited and probably requires a large scale RCT Current research is testing BA in a range of new settings
Acknowledgements thanks for listening Too many to mention Team-CASPER/COBRA and beyond study participants More info david. ekers@nhs. net Twitter @David. Ekers Disclaimer for COBRA and CASPER studies n These project was funded by the NIHR Health Technology Assessment programme. n The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HTA programme, NIHR, NHS or the Department of Health.