ISCHEMIC STROKE THROMBOLYSIS TIA Matthias Georg Ziller R

ISCHEMIC STROKE, THROMBOLYSIS & TIA Matthias Georg Ziller R 5 Neurology September 10 th 2008

Objectives 1. 2. 3. 4. Understand the clinical approach to acute stroke Understand the use of thrombolysis in acute stroke General management of stroke Approach to TIA

Why it’s important Everyday 3 rd -4 th cause of death 1 st cause of adult disability. 50, 000 new /year in Canada. 750, 000 new/year in USA. Annual 40 -44 billion (US) 30% of survivors require daily assistance

Definition Abrupt symptom onset Focal neurological deficits lasting > 24 hours � Definition changing towards tissue damage Interruption of vascular supply leads to energy failure

TYPES Lacunar 20% SAH 10% Hemorrhagic 20% Thromboembolic 10% Cardioembolic 20% Ischemic 80% ICH 10% Other 5% Unknown 25%

Risk Factors Non-modifiable � � Age Ethnicity: Blacks, Asians Male gender Family history � Stroke in first degree relative Genetics Dyslipoproteinemias Vasculopathies Cardiomyopathies MELAS, CADASIL

Risk Factors Modifiable : HTN – 3 -4 x DM – 2 -4 x with HTN SMOKING – 2 -3 x Hyperlipidemia CAD Afib – 5 -6 x Stroke , TIA , stenosis. Et. OH

Risk Factors Others: � � � High fibrinogen APL antibody Homocysteine Recent bacterial infection Sickle cell disease

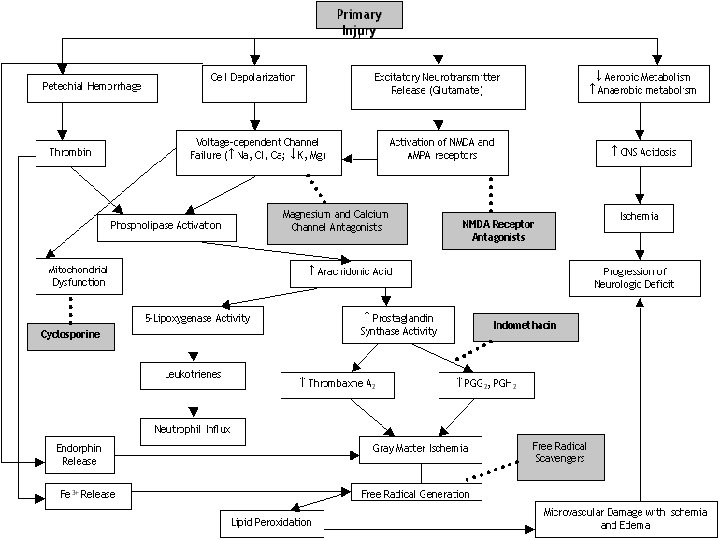
Pathophysiology Metabolically active tissue � Complete arrest of flow: � � � (15 -20% CO ) 15 sec: suppression of electric activity 2 -4 min: inhibition of synaptic excitability 4 -6 min: inhibition of electric excitability Normal CBF > 55 ml/min/100 g � � CBF<18 ml/min/100 g: electric failure CBF < 8 ml/min/100 g: membrane failure

Stroke syndromes MCA, ACA, PCA, VBS, IC Lacunar (PM, SM, HP, CD and 200 more Brain stem syndromes � Weber, Claude, Benedikt, Wallenberg. . . � Various constellations of CN and long tract findings

“ 53333 -1” Now what?

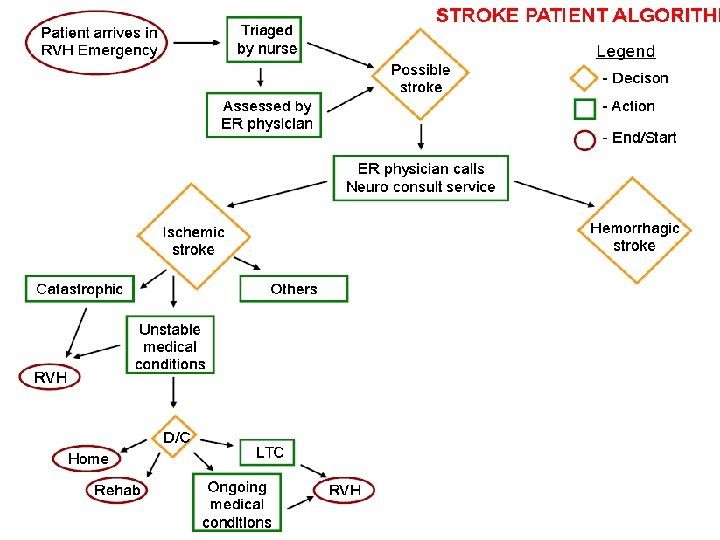
ER evaluation Immediate response ABC, Quick History: ONSET , ONSET WHEN WAS THE PATIENT LAST SEEN NORMAL ? Atypical features H/A, NECK PAIN, SZ Improvement

BEWARE OF MIMICS !
 Listen for murmurs and bruits LOC , speech")
P/E Vitals, BP both arms, Pulse(s) Listen for murmurs and bruits LOC , speech Inattention, neglect…etc CN (Pupils, visual fields, gaze, facial) Arm, leg drift, fine finger movements Sensory Dysmetria

Requisite IV lines, O 2 CBC SMA 7, ESR, PT/PTT INR: wait for it in alcoholics, possible ATC GLUCOSE EKG, ischemia markers CXR Selected patients: toxicology, b-HCG

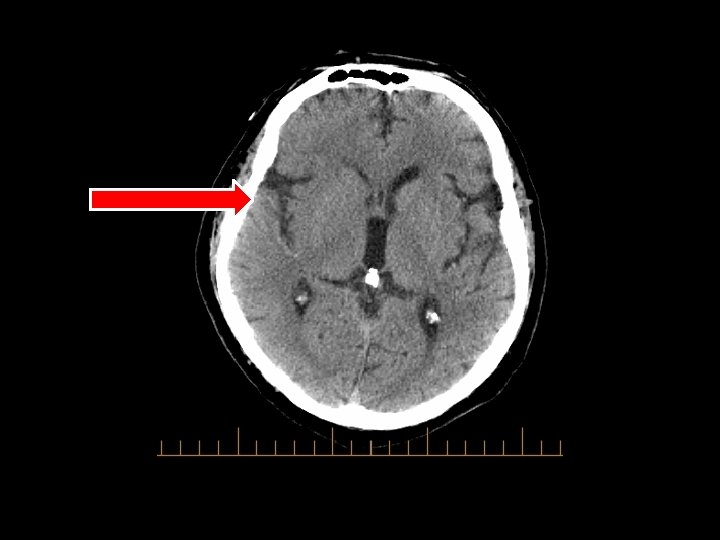
Imaging in acute stroke

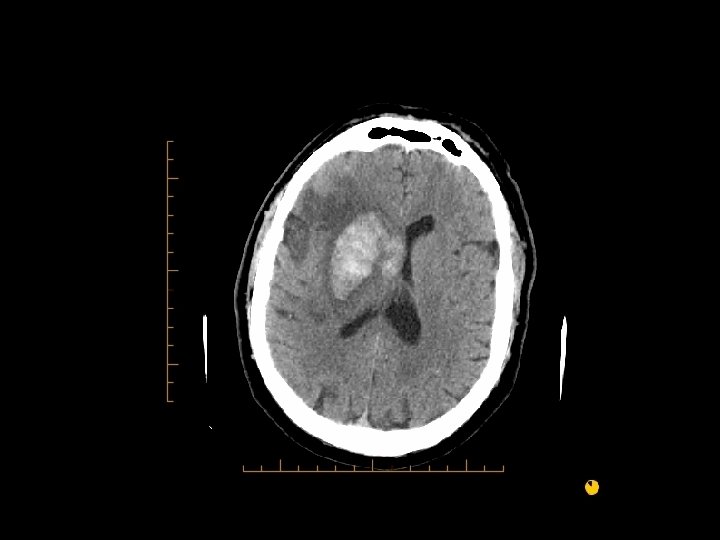
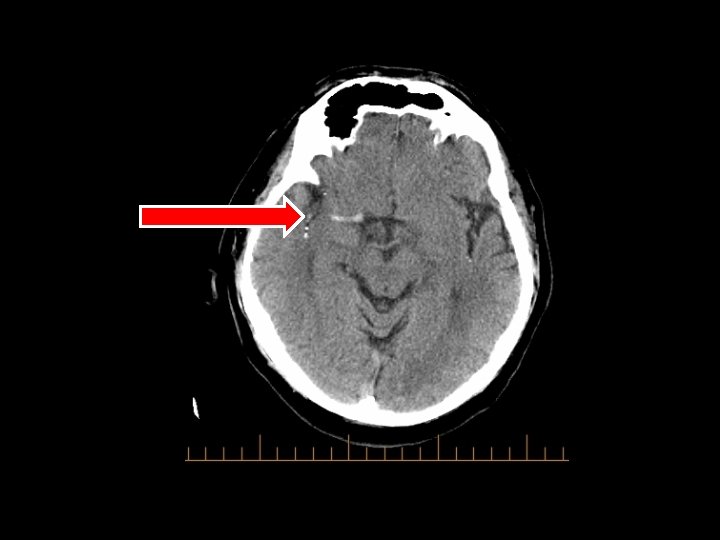
Goal Exclude hemorrhage Exclude mass lesions Assess degree of brain injury Identify the vascular lesion � Next step: CTA protocol to identify occluded vessel

First step CT scan: � Plain, � Look aim is door-to-CT 25 min for subtle signs - 50% 6 hrs Grey-white matter differentiation Sulcal effacement Obscuration of lentiform nuclei, insula MCA Parenchymal hypodensity
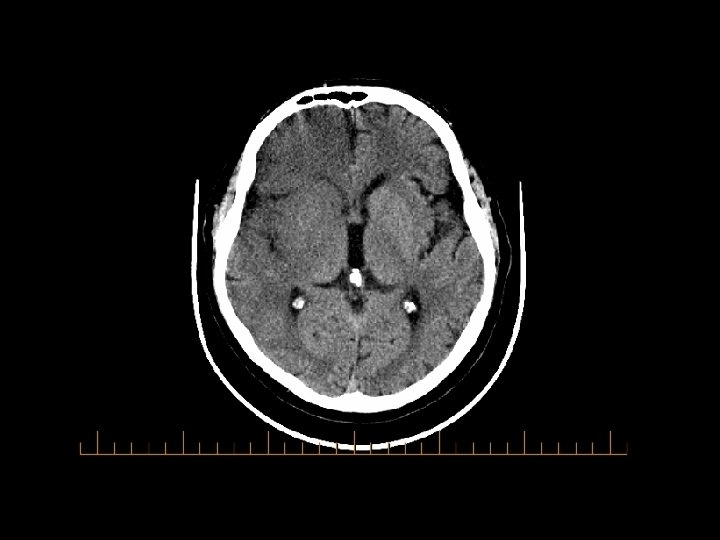

ASPECTS: Alberta Stroke Program Early CT scoring American Journal of Neuroradiology 22: 1534 -1542 (9 2001) Normal: 10 points. Substract one point for each area of attenuation. Increased disability < 7. • ▼stroke severity.

Time is brain! Saver, Stroke 2006

Indications for rt-PA Patients presenting within 3 hours of an acute ischemic stroke To be given <3 hours after stroke symptoms onset May be given <6 hours under the care of a stroke neurologist in IA protocol

Inclusion Criteria Acute ischemic stroke presenting within 3 hours of onset of symptoms No hemorrhage on CT No evidence of massive infarction or edema involving >1/3 MCA territory No midline shift (mass effect) No evidence of tumour, aneurysm or AVM

Exclusion Criteria Decreased level of consciousness Symptom onset >3 hours SAH, aneurysm, AVM, ICH, mass effect, tumour on CT, or any major hypodensity representing well-evolved infarction Stroke or serious head injury with 3 months

More exclusion criteria Previous CNS bleed History of GI/GU hemorrhage <21 days Major trauma/surgery <14 days Hematological abnormality or coagulopathy, INR >1. 7 Arterial puncture at a non-compressible site in the last 7 days
 not responding to antihypertensive therapy Pericarditis <3 months")
Even more. . HTN (BP>185/110) not responding to antihypertensive therapy Pericarditis <3 months
 RCT in 2")
NINDS: methods National Institute of Neurological Disorders and Stroke (NEJM 1995) RCT in 2 parts of 624 pts between January 1991 and October 1994 30 of 40 centers were community hospitals Included only patients within 3 h � Half within 90 minutes � Half between 90 -180 minutes Strict exclusion criteria � BP criteria � Bleeding risk � No ischemic size criteria

NINDS: methods 2 parts were independent � Part 1: early improvement 291 pts randomized to t. PA or placebo Looked at NIHSS improvement > 3 pts at 24 h � Part 2 : delayed improvement 333 pts randomized to t. PA or placebo Looked at proportion of pts who recovered with minimal or no deficits at 3 months � Looked at both outcomes for both parts (624 pts) Appropriate power for primary outcome

< 3 Hours from onset: NINDS Trial Parts A and B 16% absolute risk reduction NNT = 7 – 8 for 1 excellent or complete recovery Disability None 27 Moderate Severe 26 Death 26 21 Placebo 43 21 20 rt-PA 1 symptomatic ICH for 15 treated patients … Treatment does not decrease mortality. 17

NINDS results: bleeding Asymptomatic bleeds: no difference Symptomatic bleeds: � 6. 4%, half were fatal (occurred within first 24 hours) Benefit of t. PA occurs despite increased risk of ICH ! Later studies: Increased ICH rate associated with protocol violations.

NINDS: Conclusion ‘‘Despite an increased incidence of intracerebral hemorrhage, an improvement in clinical outcome at three months was found in patients treated with intravenous t-PA within three hours of the onset of acute ischemic stroke’’ with decreased combined severe disability and death at 3 months and a trend towards decreased mortality.

Stroke outcome with alteplase

Cochrane Review
 � Little experience with")
Community Experience Cleveland Experience Not very good results (JAMA 2000) � Little experience with t. PA � 50% protocol deviation � 15. 7% s. ICH – 15. 7% mortality Results better with time (Stroke 2003) � Institution � � � of stroke quality improvement program Less protocol deviation (19. 1%) 6. 4% s. ICH Learning curve exists and can be overcome
 CMAJ 2005 Collected")
Community Experience Canadian Experience Canadian Altepase for Stroke Effectiveness Study (CASES) CMAJ 2005 Collected 2 years of Canadian experience: � Post-marketing study (Phase IV) � 1135 patients in 60 centres (33 community hospitals)
")
CASES Similar or better results than NINDS Symptomatic intracranial hemorrhage 4. 6% (75% died) � Excellent clinical outcome in 37% at 90 days (NINDS 39%) � 154 protocol violations �

Outside the window ! Nothing to do? Don’t be sad! Or angry at someone. . . There are still ways to help your patient

Things to do Ø Admit Ø Maintain adequate tissue oxygenation, > 92 % Ø Ø Ø Common: pneumonia, hypoventilation, atelectasis 50 % of patients requiring intubation die within 1 month NPO Avoid aspiration No supportive data for hyperbaric oxygen, may be toxic Avoid hyperthermia Ø Ø Treat fever and infections No firm recommendation for cooling in 2007 AHA guidelines

Things to do Ø Ø Cardiac monitoring Ø MI and arrhythmia frequent after stroke, most often AFib Ø Arrhythmia associated with right hemispheric insular strokes Ø 24 hour monitoring recommended Blood pressure monitoring Ø Transiently elevated, optimal: 160 -200 mm Hg SBP, 70 -110 DBP Ø Lower and higher BP associated with ↑ infarct volume at 7 days Ø Lower it only if > 220/130 Ø Ø Ø or 185/110 for t. PA, use IV labetalol 10 mg q 10 -20 min Avoid hypotension, < 100 SBP associated with - outcome ASA Ø within 48 hours reduces the risk of early recurrence without a major risk of bleed and improves long-term outcome

Things to do Ø Glucose Ø Ø Seizures: Ø Ø Ø Frequent complication 5000 U bid or LMWH, safe with ASA Incontinence not uncommon in acute stroke Ø Ø 5 -8 % after stroke, prophylaxis not recommended DVT prophylaxis Ø Ø Treat hyperglycemia aggressively, frequent testing, scales and Insulin Limit use of Foleys to avoid urosepsis Pressure sores in 15 % after stroke Ø Ø Think of it Positioning, dressings, adequate nutrition

TRANSIENT ISCHEMIC ATTACKS

TIA Focal neurological deficits lasting < 24 hours New proposed definition: Rapidly resolving neurologic symptoms typically lasting less than 1 hour with no evidence of infarction on imaging Most last 5 -20 minutes It is a stroke that did not finish YET

TIA Prognostic indicator of stroke � 30 % of untreated patients have a stroke within 5 yrs � 10% within the next 3 months � 50 % of them within the first 48 hours Mortality � 5 -6 % annually, mainly by MI

TIA Prognosis Speech, motor, >10 min, age >60, diabetes Gladstone D et al. CMAJ. 2004 Mar 30; 170(7): 1099 -104.
: 1099 -104. Speech,")
TIA Risk Gladstone D et al. CMAJ. 2004 Mar 30; 170(7): 1099 -104. Speech, motor, >10 min, age >60, diabetes

TIA Prognosis Benign Timing Duration min Frequency Sensory Motor Speech Risk factors Deficit dynamics Malignant weeks ago sec – few minutes hours ago >10 multiple yes alone no no no one to few no yes HTN, DM, Mild at onset Severe at onset

High risk TIA –ABCD 2 score Age > 60 yrs =1 BP >140/90 =1 Clinical � Weakness (2 pts) � Speech without weakness (1 pt) Duration � >60 min (2 pts), � 10 -59 1 (pt) � <10 (0 pts) Diabetes = 1 point Rothwell PM et al-Lancet 2005

High risk TIA –ABCD score Rothwell PM et al-Lancet 2005

DWI restriction common in TIA ~50% of all TIA’s associated with permanent damage. Especially if it lasts > 1 hour. Even brief symptoms cause areas of permanent injury Kidwell C et al. Stroke 1999; 6: 1174 -1180. Couttts SB et al. Annals of Neurology 2005; 57: 848 -854

TIA- Evaluation Detailed history CT head/MRI brain Metabolic parameters ECG- AF Carotid doppler/MRA/CTA Echo

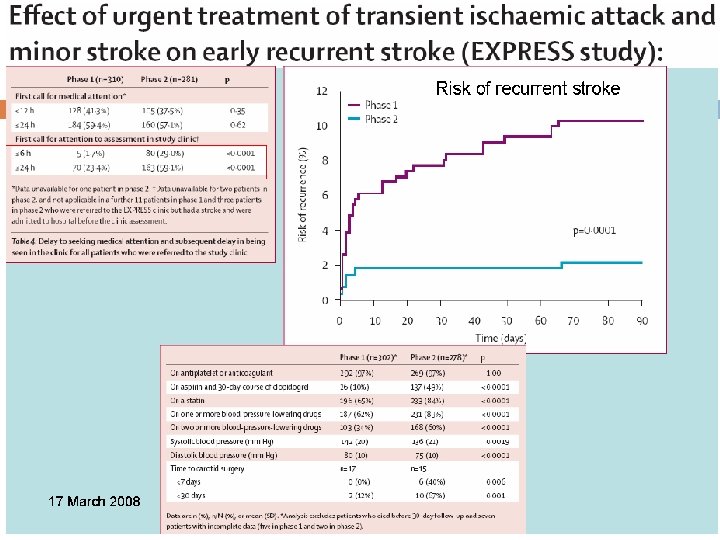
Management Admission for malignant TIA Urgent evaluation Antiplatelets Statin Control risk factors CEA or stenting early

Thank you: On the shoulders of giants: � Mike Sidel, Alexandre Poppe, Adel Al-Hazzani, Dr Minuk and Dr Cote, Charles Miller Fisher … The Patient Study Group and …
- Slides: 58