IRRITABLE BOWEL SYNDROME Barbara L Slee M D

IRRITABLE BOWEL SYNDROME Barbara L. Slee, M. D.

IBS • • Epidemiology and pathophysiology Symptoms and signs of Dx Appropriate Work-up Treatment

Definition of IBS • • Benign GI disorder Chronic abdominal pain Altered bowel habits Absence of organic causes

Epidemiology • • • Incidence: 10 -15% pop. Most common GI disorder 2: 1 female/male Younger patients 2 nd highest cause of missing work $2 -8 billion

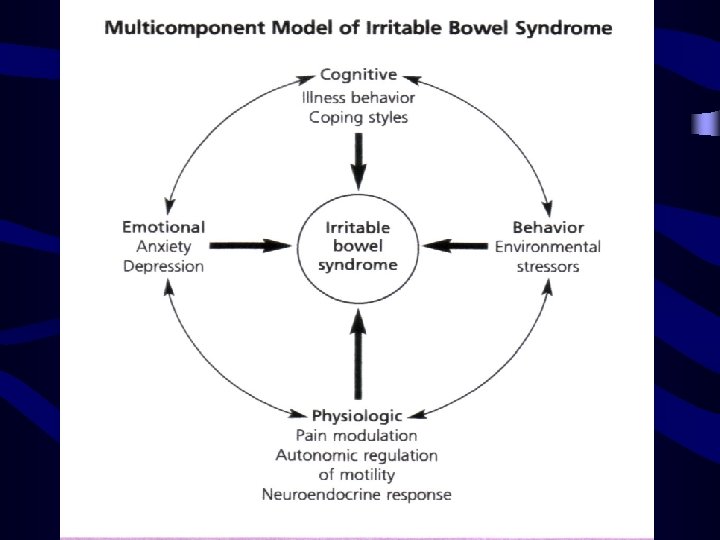
Pathophysiology • Altered GI motility • Visceral afferent hypersensitivity • Psychosocial dysfunction

Clinical Presentation?

Clinical Presentation • • • Chronic episodic abdominal pain Cramping Pain relieved by defecation Looser, more frequent stools Diarrhea, constipation, or alternating Mucous in stool

Clinical Presentation • • • Bloating, gas Dyspepsia, Nausea Atypical chest pain Symptoms worse during stressful time Normal Exam

Diagnosis Criteria • Manning • Rome II – 12 or more wks of abd pain – +2 or more of following • Relieved by defecation • Change in frequency • Change in form

• Alarm symptoms or Red Flags?
 • • Anemia Family history colon CA or IBD Fever")
Alarm Symptoms (Red Flags) • • Anemia Family history colon CA or IBD Fever Nocturnal symptoms
 • • • Bleeding >10 lb wt loss Recent Antibiotic Severe")
Red Flags (con’t) • • • Bleeding >10 lb wt loss Recent Antibiotic Severe chronic diarrhea > age 50

Work-up for IBS • • 27 y/o female pt Intermittent, crampy abdominal pain Stool urgency, relief of pain with BM No alarm findings • What studies?

REC. W/U for IBS • Pretest probability of organic disease <1% • Same in healthy controls

Diagnostic Studies in IBS: • • • CBC, Chem 14 Stool O&P – if diarrhea, endemic infection +/- TSH – severe diarrhea +/- hemoccult +/- ESR (younger pt) Colonoscopy – age >50

Screen for Celiac Dz • Incidence in IBS = 5% • Healthy controls <1% • If diarrhea predominant sx – Antigliadin Ab, antimysial Ab – Upper endoscopy with Biopsy if suspicious and Abs negative

Treatment • How do you want to Treat your patient?

Treatment: • • Doctor –patient relationship Education Reassurance Chronic benign nature

Dietary – Food exclusions • • • Lactose Fructose Foods that increase flatulence Caffeine Any food they find increases their sxs

Medication: • • Adjunct only Avoid chronic use Use based on predominant symptoms Lack of convincing evidence of efficacy

Pain Sx: • Anti-spasmotics – Bentyl – Hyoscymine – Levsin, Symax • TCA’s – Low dose – Decrease visceral sensitivity, motility, secretions
 prn Cholestyramine (questran) Ondansetron (Zofran) 5 HT")
Diarrhea predominant sx: • • Loperimide (lomotil) prn Cholestyramine (questran) Ondansetron (Zofran) 5 HT 3 antagonist Alosetron (Lotronex) 5 HT 3 antagonist
 HT 4 Agonist –")
Constipation predominant sx: • Fiber 25 g/day • Tegaserod (Zelnorm) HT 4 Agonist – Studies valid for efficacy in women only

Cost of Medication • Zelnorm 2 mg or 4 mg • Lotronex 1 mg • Zofran 8 mg $100/mo 252/mo 1277/mo

Pychotherapy: • • • Symptoms unresponsive Impair health related quality of life Co-morbid psychological diagnosis History of Physical or sexual abuse Learned patterns of illness behavior

Psychotherapy • Mental health professional part of Treatment Team • No one Psych therapy modality superior

Summary • • Etiology is unclear IBS pathophysiology is multifactorial Diagnosed by H&P Requires minimal lab evaluation in absence of Alarm symptoms

Summary • Treatment is first reassurance and nonpharmacological measures • Pharmacotherapy is used when needed and for brief periods only

Handouts • Text of lecture • Criteria for Diagnosis of IBS • Treatment Strategy Chart for IBS from NEJM, Irritable Bowel Syndrome: Review Article Nov. 27, 2003 • Cover Article from AFP Nov. 15, 2002, Management of Irritable Bowel Syndrome by Anthony Viera and Steve Hoag

References • 1. Evidence-Based Position Statement on the Management of Irritable Bowel Syndrome in North America; ACG, American Journal of Gastroenterology, Vol. 97 No. 11 Suppl. , 2002 • 2. Systematic Review on the Management of Irritable Bowel Syndrome in North America; L. J. Brandt, M. D. , chairman, David Bjorkman, M. D. , M. Brian Fennerty, M. D. et. al, The American Journal of Gastroenterology, Vol. 97, No. 11, Suppl. , 2002

References • 3. Schoenfeld, MD, Philip, Efficacy of Current Drug Therapies in Irritable Bowel Syndrome: What Works and Does Not Work. Gastroenterology Clinics of North America, 34 (2005) 319 -335 • 4. Anthony Viera, Steve Hoag, Lt. MC. Management of Irritable Bowel Syndrome, AFP Nov. 15, 2002 • 5. AGA Guideline: Irritable Bowel Syndrome, Gastroenterology 2002; 123: 2105

References • 6. Anddrew B. chun, M. D. , Steven Desautels, MD, Arnold Wald, MD. Clinical Manifestations and diagnosis of Irritable Bowel Syndrome, Up. To. Date. Online 13. 2 • 7. Sanders DS, Carter MJ, et al. Irritablae Bowel Syndrome Was significantly Associated with Celiac Disease: Update in Gastroenterology and Hepatology. Annals of Internal Medicine, Sept. 7, 2004.

Other Interesting Reading: • 1. The Role of Food Intolerance in Irritable Bowel Syndrome, Raichard Lea, Peter Whorwell, MD. Gastroenterology Clinics of North America 34 (2005) 247 -255 • 2. Probiotics: An Ideal Anti-inflammatory Treatment for IBS? Editorial, Gastroenterology Vol. 128 No. 3
- Slides: 34