Iron Deficiency Anemia By Kristi Cockrell Why I

Iron Deficiency Anemia By Kristi Cockrell

Why I chose this topic Interested in the disease and management Younger brother is on the verge of IDA Family wanted to learn more about IDA in order to help my brother

Overview of the presentation Background of the disease Describe Iron Deficiency Anemia Causes and symptoms Who IDA affects Diagnosis of IDA management Nutrition’s role in the condition Ethical Dilemmas with MD and Nutrition Summary What you should know

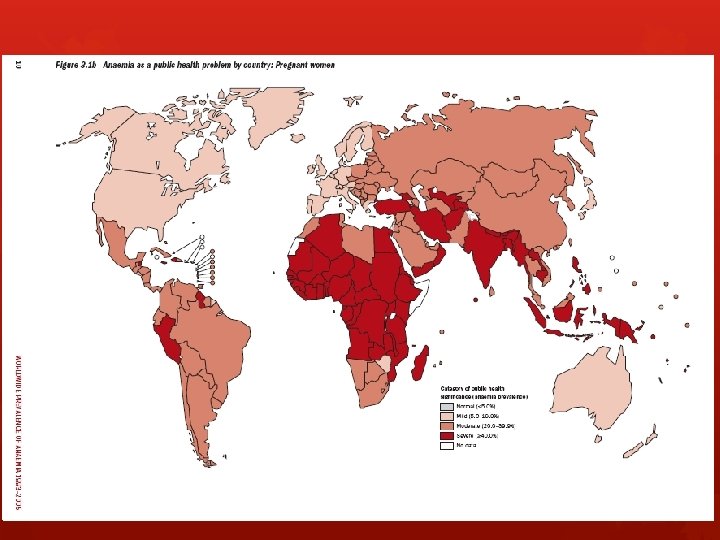
Historical background Nutritional anemia was defined in 1968 World health organization “A condition in which the hemoglobin content of the blood is lower than normal as a result of a deficiency of one or more essential nutrients, regardless of the cause of such deficiency. “ Ran a series of studies in pregnant women Found iron deficiency the most prevalent 3. 5 billion iron deficient people worldwide Vast majority in developing countries

What is Iron Deficiency Anemia? Most common nutritional deficiency around the globe Advanced stage of iron deficiency (even more common) Anemia is when your body does not have enough healthy red blood cells Iron is an important building block for red blood cells Body is low on iron Not enough red blood cells Cells are too small

Red Blood Cells Bring oxygen to body tissues Made in the bone marrow Move through body for 3 -4 months Parts of the body then remove old blood cells Iron is a key factor No iron = blood cannot carry oxygen efficiently Iron is normally absorbed through food or old red blood cells

Causes of IDA Lose more blood cells and iron than your body can replace Body is not efficient in absorbing iron Not eating enough iron rich foods Body needs more iron than normal Pregnant Breastfeeding Bleeding: Heavy, long or frequent menstrual periods Cancer in the esophagus, stomach or colon The use of aspirin, ibuprofen, or arthritis medicine for a long period of time

Causes of IDA Peptic ulcer disease Diet: Celiac disease Crohn’s disease Gastric bypass surgery Taking too many antacids that contain calcium Unhealthy diet Strict vegetarian Elderly Do not get a full diet

Symptoms of IDA May have no symptoms if the anemia is mild Symptoms are mild at first and develop slowly Grumpy Blue color to the whites of eyes More weak or tired than usual (or when Brittle nails exercising) Light-headedness when standing Headaches Problems concentrating Pale skin Fatigue Shortness of breath Chest pain Sore tongue

Symptoms of conditions that cause IDA Dark, tar colored stools or blood Heavy menstrual bleeding Pain in the upper belly (from ulcers) Weight loss (in people with cancer)

IDA in infants and toddlers/Developmental loss Signs of IDA Poor appetite Slowed growth or development Behavioral problems Children < 5 yrs 25% or higher in low or middle income countries Adverse psychomotor, cognitive, and socioemotional development Animal studies: suggest IDA may affect neurological development

IDA in infants and toddlers/Developmental loss Infants Born preterm or with low birth weight Mothers who are anemic or diabetic Study of neonates exposed to low iron in utero IDA early in life can lead to auditory and visual system deficits—may not be responsive to iron supplementation IDA during rapid brain growth may be irreversible Toddlers Studies link IDA to cognitive difficulties and poor fine and gross motor development Studies show that some developmental delays can be reversed with iron therapy

IDA in infants and toddlers Increased risk of IDA in infacy Maternal ID Early cord clamping Early or prolonged introduction of cow’s milk Iron-insufficient complementary food Vulnerability increases at 6 months Prenatal stores have depleted Need > breast milk can provide

IDA in adults > 3000 mg elemental iron in the body Males > Females (due to blood loss during menses, pregnancy and lactation) 2/3 heme iron 1/3 non-heme Ferritin or hemosiderin About 20 mg is recycled daily into the bone marrow Additional 1 -2 mg/day for iron loss from urine, sweat and stool

IDA in adults Daily elemental iron requirement: Children > 5 yrs of age, men and postmenopausal women : 10 mg Young, non-pregnant women: 20 mg Pregnant or lactating women: 30 mg patients who mal-absorb iron (gastric bypass): > 30 mg.

How to Diagnose Blood tests: Hematocrit and Hemoglobin RBC indices Testing iron levels: Bone marrow exam (rare) Iron binding capacity (TIBC in the blood) Serum ferritin Serum iron level Testing for the cause: Colonoscopy Upper endoscopy Fecal occult blood test

Diagnostic criteria Red blood cells With IDA red blood cells are smaller and paler in color Hematocrit Normal levels: Women 35 -45% Men 39 -50% Lower than normal hemoglobin levels 13. 5 -17. 5 g/d. L of blood for men 12 -15. 5 g/d. L of blood for women Lower than normal level of ferritin
 Oral Intravenous Injection in the muscle Iron-rich")
How to manage IDA Supplements (ferrous sulfate) Oral Intravenous Injection in the muscle Iron-rich foods: Chicken and turkey Dried lentils, peas Egg yolks Fish Meats (liver is the highest source) Peanut butter Soy beans Whole-grain bread

How to manage IDA Iron-rich foods: Oatmeal Raisins Prunes and apricots Spinach, kale and other greens Hematocrit should return to normal after 2 months of iron therapy 6 -12 months to replace iron stores in bone marrow With treatment = outcome is likely to be good Does depend on cause

How to manage IDA Iron tablets are recommended between meals or at bedtime Avoid alkalinizing effect of food Take advantage of peak gastric acid production Adults: daily dose of 150 -200 mg of elemental iron One ferrous sulfate tablet 3 times/day Each tablet contains approximately 60 mg May fully correct after 4 weeks if more iron is needed to replenish this regimen may be recommended for several additional months Gastrointestinal discomfort Self discontinue Amount of absorbed iron decreases as the iron deficiency is corrected

Nutrition’s Role Huge role in preventing and treating IDA Heme iron: red meat and liver (full of hemoglobin and myoglobin Non-heme iron: cereals, egg yolk and green, leafy vegetables (not efficiently absorbed) Vitamin C increases iron absorption Increase citrus fruit intake Tea inhibits iron absorption 1 -2 hours after a meal Remove tea from diet Too much dietary fiber can lead to mal-absorption of iron

Opinion on management of IDA Eat a healthy, well balanced diet Foods that contain iron Red meat Fish Soy Egg yolk Dark leafy greens Breastfeed infants until age 1 Feed infants age 6 -12 months iron fortified infant food Children should not drink too much cow’s milk Talk to a doctor if you notice any of the signs Take elemental iron supplementation if needed or prescribed by our doctor

Ethical Dilemmas between MD and Nutrition 10%--average absorption of iron in medicinal form Patients should not take iron supplements within 1 -2 hours of antacids Iron absorption is delayed with the intake of: Medications that reduce stomach acid Milk Carbonated soft drinks Multivitamin pills Should never be recommended as sole therapy for IDA

Summary More common in infants, toddlers, children, pregnant women and elderly Defined in 1968 by the WHO Most common nutritional deficiency in the world Iron is the building block for red blood cells Symptoms may not show if anemia is mild Symptoms develop slowly Can cause slowing of cognitive development in infants and toddlers Developmental delays can possibly be reversed through iron therapy Eating a well-rounded, healthy diet should supply your body with the iron needed Iron absorption can be delayed through the intake of certain medications and foods

What you should know History of IDA Causes of IDA Symptoms of IDA Effects of IDA in infants, toddlers, children and adults Usual recommended doses for iron therapy Diagnostic criteria How to manage IDA Nutrition’s role in the disease Ethical dilemmas with MD and Nutrition

Any Questions? ?









- Slides: 37