IRON DEFICIENCY ANAEMIA BY DR FATMA ALQAHTANI CONSULTANT

IRON DEFICIENCY ANAEMIA BY DR. FATMA ALQAHTANI CONSULTANT HAEMATOLOGIST

PER CENT OF INFANTS 20 FORMULA 10 0 BREAST MILK 20 10 0 COW’S MILK 20 10 0 4 AGE 6 IN 9 12 MONTHS Percentage of infants with iron deficiency, defined as serum ferritin below 10µ g/l. after feeding iron-supplemented formulas, breast milk and cow’s milk.

Factors which affect iron content at birth ------------------------------------------------------------------------------- Iron content --------------------------------------------------- Increased Decreased ------------------------------------------------------------------------------- Tissue iron Blood Volume High birth weight Haemolytic disease High birth weight Late cord clamping Low birth weight Early cord clamping Haemorrhage from cord or placenta Materno-fetal transfusion Feto-material transfusion Cord haemoglobin Feto-fetal transusion Growth retardation Maternal anaemia Maternal hypoxia Feto-fetal transfusion Pre-term infant Haemolytic disease
 --------------------------------------------------------------------------------- Daily Loss Requirement Total Loss for Growth")
Daily Iron Losses and Requirements (mg) --------------------------------------------------------------------------------- Daily Loss Requirement Total Loss for Growth (= Requirement) Urine, skin, menses Faeces, etc. -------------------------------------------------------------------------------- Infant (0 -4 months) (5 -12 months) Child Adolescent male Adolescent female Menstruating female Adult male Post menopausal female 0. 5 0. 9 0. 9 1. 0 1. 9 0. 5 0. 9 0. 5 1. 0 1. 8 2. 4 2. 8 0. 9 ------------------------------------------------------------------------------- N. B: Average daily requirement during pregnancy is 3. 0 – 4. 0 mg.
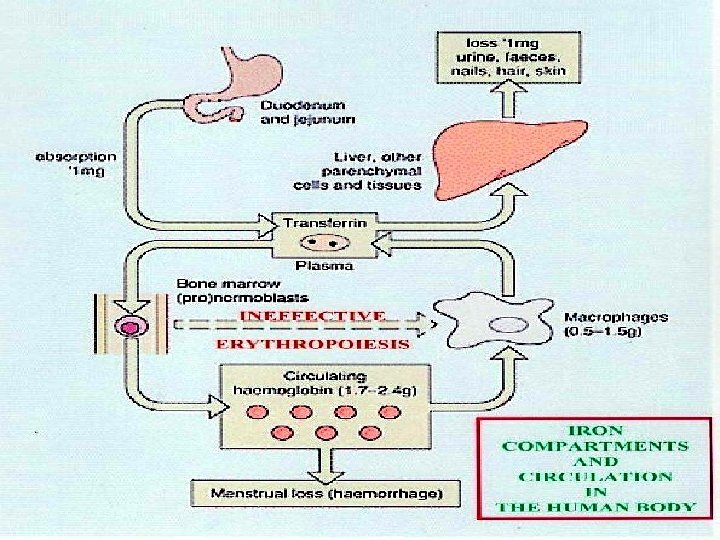

IRON ABSORPTION Favored by • Dietary factors: Increased Haem iron Increased animal iron Ferrous iron salts • Luminal factors: Acid p. H (e. g. gastric HCl) Low molecular weight soluble chelates (e. g. Vit. C, sugars, amino acids) • Ligand in meat (unidentified) • Systemic factors: Iron deficiency Increased erythropoiesis Ineffective erythropoiesis Pregnancy Hypoxia Reduced by Decreased haem iron Decreased animal iron Ferric iron salts Alkalis (e. g. pancreatic secretions) Insoluble iron complexes (e. g. phytates, tannates in tea, bran) Iron overload Decreased erythropoiesis Inflamatory disorders
 Normal normal")
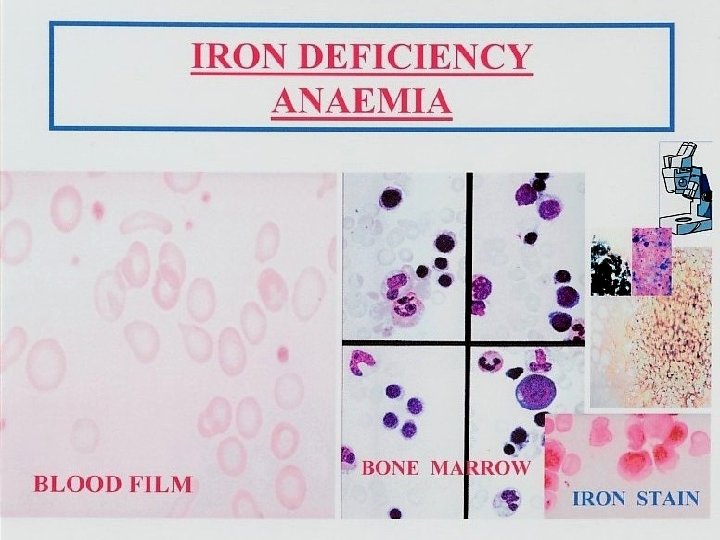
Normal Latent Iron Deficiency Anaemia Red cell iron (peripheral film And indices) Normal normal hypochromic, microcytic MCV↓MCHC↓ Iron stores (bone marrow Macrophage iron +++ - + 0 0 The development of iron deficiency anaemia. Reticuloendothelial (macrophage) stores are lost completely before anaemia develops.

serum iron Serum iron binding capacity normal iron deficiency anaemia of chronic disorders iron overload 0 10 20 30 40 50 60 70 80 90 100 µ mol/l The serum iron and unsaturated serum iron binding capacity in normal subjects, iron deficiency, the anaemia of chronic disorders and iron overload. The total iron binding capacity (TIBC) is made up by the serum iron and the unsaturated iron binding capacity.

Normal Iron Depletion Iron Deficient Erythropoiesis Iron Deficiency Anaemia Iron Stores Erythron Iron RE Marrow Fe (O-6) Transferrin IBC (µmol/l) Plasma Ferritin (µg/l) Iron Absorption Plasma Iron (µmol/l) Transferrin Saturation (%) Sideroblasts (%) RBC Protoporphyrin (µg/dl RBC) Erythrocytes 2 -3+ 60± 5 100± 60 Normal 20± 9 35± 15 40 – 60 30 normal 0 -|+ 65 20 ↑ 20 30 40 -60 30 normal 0 70 10 ↑ <10 <15 <10 100 normal 0 75 <10 ↑ <7 <10 200 Microcytic and hypochromic The sequence of changes induced by a gradual reduction in the iron content of the body.
 Iron deficiency PROTOPORPHYRIN Sideroblastic anaemia (b) Chronic inflammation or malignancy HAEM +")
IRON (a) Iron deficiency PROTOPORPHYRIN Sideroblastic anaemia (b) Chronic inflammation or malignancy HAEM + GLOBIN Thalassaemia ( α or β ) HAEMOGLOBIN The causes of a hypochromic microcytic anaemia include: • lack of iron (iron deficiency) or of iron release from macrophages to serum (anaemia of chronic inflammation or malignancy) • Failure of protoporphyrin synthesis (sideroblastic anaemia) • Failure of globin synthesis (α or β–thalassaemia). Lead also inhibits haem and globin synthesis.

Hypochromic and/or Microcytic Anaemia Serum Fe Normal Reduced Hypoferraemia Bone Marrow Macrophage Iron Absent Increased OR Serum Ferritin IRON DEFICIENCY ANAEMIA OF CHRONIC DISORDERS Low Normal or Increased Hemoglobin Electrophoresis, etc THLASSEMIA HEMOGLOBINOPA THIES (S, C, D, E) Serum Fe Increased Hyperferraemia Bone marrow Sideroblast Fe Increased SIDEROBLASTIC ANAEMIA CONGENITAL ACQUIRED

Failure of response to oral iron ------------------------------------------------------------------------------- • • Continuing haemorrhage Failure to take tablets Wrong diagnosis – especially thalassaemia trait, sidroblastic anaemia Mixed deficiency – associated with folate or vitamin B 12 deficiency Another cause for anaemia – e. g. malignancy, inflammation Malabsorption – this must be extremely severe Use of slow – release preparation
- Slides: 16