Investigations In Urology By Ahmed Hakim Abdel Gawad

“Investigations In Urology” By: Ahmed Hakim Abdel Gawad lecturer of urology faculty of medicine, Minia University

Investigations of urology may be divided into : 1 -Imaging. Radiological investigations. . Ultrasonography. . Computed tomography. Magnetic resonance imaging 2 - Laboratory 3 - instrumental 4 - Urodynamic studies

Radiological investigation may include : Plain X-ray urinary tract intravenous urography Cystograms Voiding cystouretheragraphy Ascending urethrogram Angiography Descending nephrostogram Ascending ureterogram

Plain X- ray Urinary Tract A plain film of the abdomen, frequently called a KUB film, is the simplest uroradiologic examination Indications ? ? ? Renal complaints Urine changes preoperative

Skeleton Soft tissue shadow Stones NO URINARY TRACT ANATOMY RADIOLUCENT STONE

Intravenous Urography The collecting structures of the kidneys, ureters, and bladder can be demonstrated radiologically with contrast media by Intravenous Urography The IVU, also known as excretory urography (EU), IVU can demonstrate a wide variety of urinary tract lesions (is simple to perform, and is well tolerated by most patients ).

Intravenous Urography IVU/ intravenous pyelogram is the classic modality of imaging the entire urothelial tract from pyelocalyceal system through the ureters and bladder – Excellent for identifying small urothelial lesions as well as the severity of obstruction from calculi – Provides anatomical and qualitative functional information about the kidneys
 Films")
Technique of IVU Patient preparation Radio-opaque dye (water soluble iodinated compounds like urographin) Films taken at 5, 10 , 15 , 30, minutes , may be late films and postvoid. Phases: Nephrographic phase Pylographic phase Cystographic phase

IVP GOOD EXCRETORY FUNCTION OF THE LEFT KIDNEY NON-VISUALIZED RIGHT KIDNEY THE LEFT KIDNEY SHOWS HYDRONEPHROSIS UPJ OBSTRUCTION

IVU SHOWING GOOD EXCRETORY FUNCTION OF BOTH KIDNEYS HORSE-SHOE KIDNEY
 Pregnancy Renal insufficiency ( serum creatinine")
Contraindications of IVU Hypersensitivity to dye (iodine ) Pregnancy Renal insufficiency ( serum creatinine more than 2. 8 or blood urea 120 ) Thyrotoxicosis Liver failure Heart failure

Cystography Permits imaging of an opacified urinary bladder after retrograde instillation of contrast media through a urethral or suprapubic catheter Imaging is performed to demonstrate a suspected urine leak, either from traumatic bladder rupture or after bladder surgery Can also demonstrate a presence of a fistula between the bladder and vagina or to characterize bladder diverticuli

CYSTOGRAM CENTRAL BASAL SEMILUNAR SMOOTH FILLING DEFECT BPH

AN IVU SHOWING GOOD EXCRETORY FUNCTION OF BOTH KIDNEYS FILLING DEFECT IN THE RT-SIDE OF THE BLADDER CANCER BLADDER

CYSTOGRAM MULTIPLE DIVERTICULAE URETHRAL CATHETER. BPH

Retrograde Urethrography Complete evaluation of the urethra includes n both antegrade and retrograde urethrography Used for evaluating a suspected traumatic urethral injury or urethral stricture Can also be useful for diagnosis of a urethral diverticulum in females

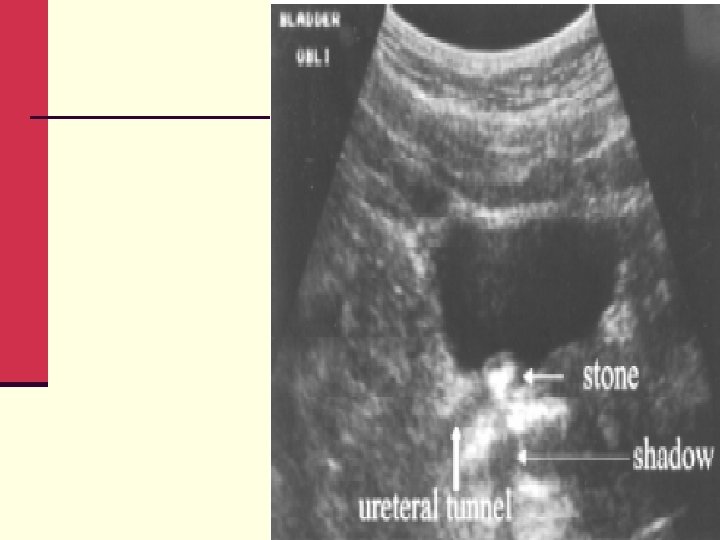
Ultrasonography cheap widely available no radiation no contrast operator dependent do not show the ureter

U/S bladder mass
 Scan CT DETAILED ANATOMY RENAL FUNCTION EXPENSIVE NEEDS CONTRAST")
Computed tomography (C. T ) Scan CT DETAILED ANATOMY RENAL FUNCTION EXPENSIVE NEEDS CONTRAST IRRADIATION USED IN TUMORS TRAUMA STONES CT SHOWING RENAL MASS
")
Multidetector C. T (C. T kub )

MRI Can be generally used in place of a CT scan n when renal insufficiency or contrast allergy prohibits the use of CT scan

Urine Analysis Method of collection Midstream sample clean catch in adult male and female suprapubic aspiration in neonates and infants
 Analyzed within 2 hours of collection Should be")
First morning voiding (most concentrated) Analyzed within 2 hours of collection Should be Free of debris or vaginal secretions
 Microscopic Examination Culture ü")
Types of Analysis Macroscopic Examination ü Chemical Analysis (Urine Dipstick) Microscopic Examination Culture ü ü Cytological Examination ü ü

Macroscopic Examination Color: normally amber yellow , but may be Red urine , may be due to : 1 - hematuria 2 - hemoglubinuria 3 - myoglobinuria 4 - drugs as rifampcin

Aspect of urine Normally , urine aspect is clear , but may be turbid due to 1 - pyuria 2 - phsphaturia 3 - chyluria

Chemical Analysis Glucose Bilirubin Ketones Specific Gravity Blood p. H Protein Urobilinogen Nitrite Leukocyte Esterase
 + (250 mg/d. L) ++")
The Urine Dipstick: Glucose Negative Trace (100 mg/d. L) + (250 mg/d. L) ++ (500 mg/d. L) +++ (1000 mg/d. L) ++++ (2000+ mg/d. L)
 chronic")
The Urine Dipstick: Specific Gravity 1. 000 1. 005 Significance Diabetes insipidus (1002) chronic renal failure low fixed (1010) 1. 010 1. 015 1. 020 1. 025 1. 030
: metabolic acidosis, high-protein diet -")
p. H Significance - Acidic (less than 4. 5): metabolic acidosis, high-protein diet - Alkaline (greater than 8. 0): renal tubular acidosis (>5. 5), UTI 5. 0 6. 5 7. 0 7. 5 8. 0 8. 5

Protein Dip strips can be used to determine the presence off more than 10 mg/dl Persistent proteinuria detected in this manner will require quantitative estimation Significant proteinuria is excretion of more than 1 gm/ 24 hrs Negative Trace + (30 mg/d. L) ++ (100 mg/d. L) +++ (300 mg/d. L) ++++ (2000 mg/d. L)

Causes of false positive results Concentrated urine High RBCs or WBCs Vaginal secretions and epithelial cells Transient proteinuria , may be due to sever muscular exercise or fever Persistent proteinuria may be due to Nephrotic syndrome Glomerulopathy Tumors Multiple myeloma
 ++ (moderate)")
Leukocyte Esterase Significance - Pyuria - Acute inflammation Negative Trace + (weak) ++ (moderate) - Renal calculus +++ (strong)

Nitrite Significance Gram negative bacteriuria Negative Positive

Microscopic Examination General Aspects Preservation - Cells and casts begin to disintegrate in 1 - 3 hrs. at room temp. - Refrigeration for up to 48 hours Types of microscopy - Phase contrast microscopy - Bright field microscopy
 (400 x) > 3 erythrocytes > 5")
Abnormal Findings Per High Power Field (HPF) (400 x) > 3 erythrocytes > 5 leukocytes > 10 bacteria

RBCs

WBCs

Bacteria

Crystals Urate Ø Uric acid Calcium Oxalate Triple Phosphate Amino Acids Cystine Ø Ø Ø

Important lab blood tests Serum creatinine is the product of the metabolism of creatine in skeletal muscles , normally excreted only by the kidneys. Normal values : 0. 6 -1. 2 mg /dl The creatinine levels remains within normal until Approximately 50% of renal function has been lost

Blood urea Urea is the primary metabolite of protein metabolism and synthesized in the liver. Urea is excreted entirely by the kidneys by glomerular filtration but it is reabsorbed by the renal tubules. Normal blood levels 20 - 40 mg/dl Blood urea level is not highly specific to the kidneys bec. It is influenced by many factors as : liver condition Hydration status of the patient Dietary protein intake

Endoscopic - urethroscopy - cystoscopy - ureteroscopy

Urodynamic studies Is a diagnostic tool for the identification and measurement of physiologic and phologic parameters involved in the storage, transportation and evacuation of urine. Include uroflowmetry cystometry urethral pressure profile electromyography

- Slides: 49