Investigations and Treatment for Stable Coronary Artery Disease

Investigations and Treatment for Stable Coronary Artery Disease Dr Reto Gamma Consultant Cardiologist Essex CTC and Broomfield Hospital September 2017
 57 year old patient n Cholesterol 7. 5 mmol/l")
Case report Mr NH (2006) 57 year old patient n Cholesterol 7. 5 mmol/l n Hypertension 170/95 mm. Hg n DM II: Hb. A 1 c 7. 8%, on Metformin 500 mg BD n Mild angina on exertion, borderline positive ETT in 2006 n Medication optimized and referred for angio n

Severe lesion in PLV BP now 130/80 mm. Hg, TC 4. 5 mmol/l, HDL 2. 9 mmol/l, Hb. A 1 c 7. 5% Otherwise asymptomatic

What is this patient’s risk of suffering a heart attack or death due to his coronary artery disease? Annual mortality? Annual rate of non-fatal infarction?

What is the prognosis of patients suffering from stable angina? n n Annual mortality 0. 9 -1. 4% Annual rate of nonfatal infarction 0. 5 -2. 6%

Management n Patient treated with higher dose of Metformin and Atorvastatin and discharged 2006 n Presents 6 years later, in 2012, with inferior myocardial infarction n What has happened?

Severe lesion in PLV, Unchanged for 6 years Culprit lesion

Another Case report 59 year old man n Smoker, cholesterol 7. 4 mmol/l n Presented with non-cardiac chest pain to RACPC n Discharged by registrar with reassurance that CP is not cardiac n Presents a week later with heart attack n

JBS 3 risk

JBS 3 risk

Revscularisation is for Symptoms, if you want to improve a patient’s prognosis, treat their risk! n n Life style changes Diabetes control Cholesterol lowering Blood pressure control

Diabetes control Use drugs with proven benefit in reducing cardiovascular events: n Metformin n SGT 2 inhibitors (Empagliflozine/Dapagliflozine) n Liraglutide

Incidence of heart attacks is falling

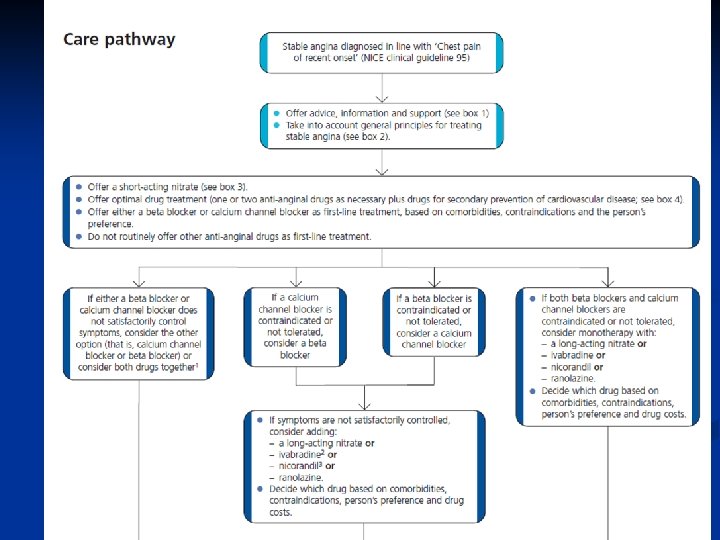
Treating cardiovascular risk Chest pain Treating symptoms

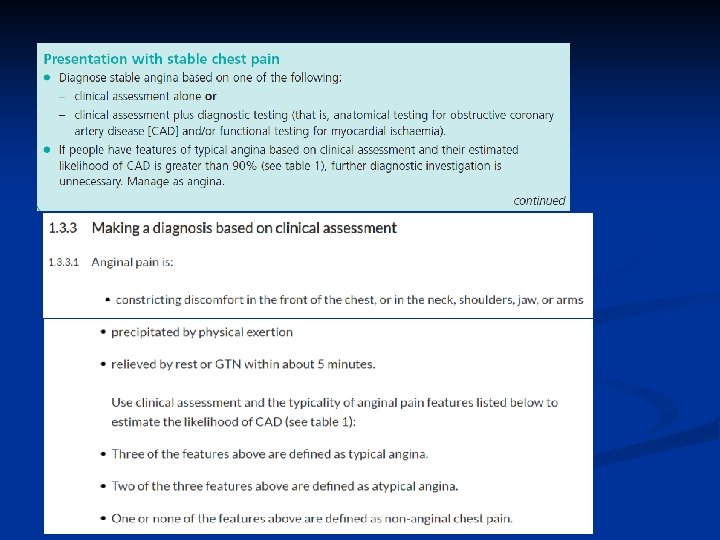
What is angina?

Most patients seen in RACPCs have non-typical angina

William Heberden‘s description of Angina pectoris

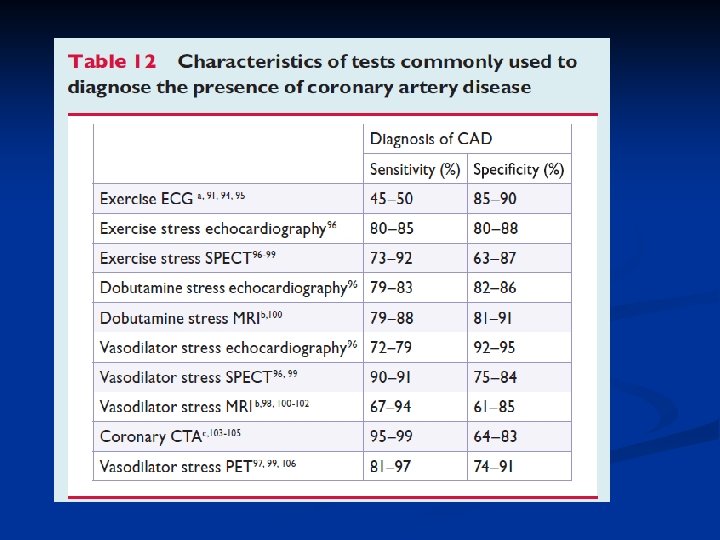
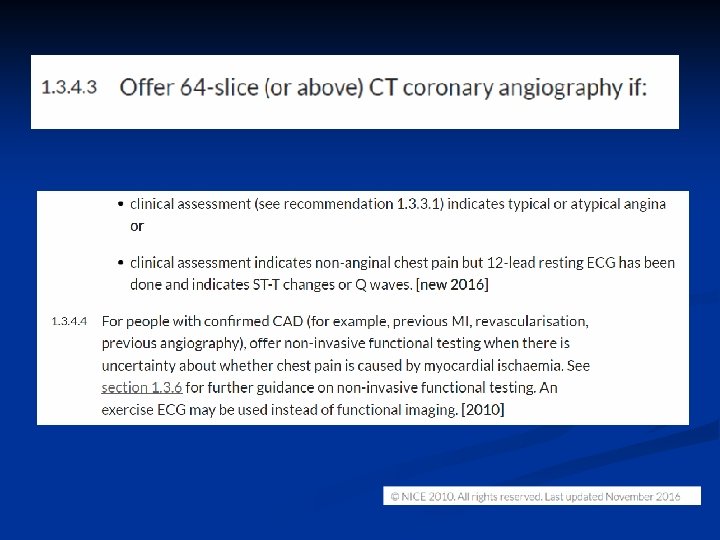
Functional versus Anatomical Test Anatomical: n Invasive coronary angiogram n CT coronary angiogram Functional: n (Exercise tolerance test) n Dobutamine/exercise stress echocardiogram n Perfusion scan (SPECT/MIBI) n PET

The ischaemic cascade

Patients referred for tests after clinical assessment RACPC audit Dr Nadine Hiari, Adam Langley, Dr Reto Gamma

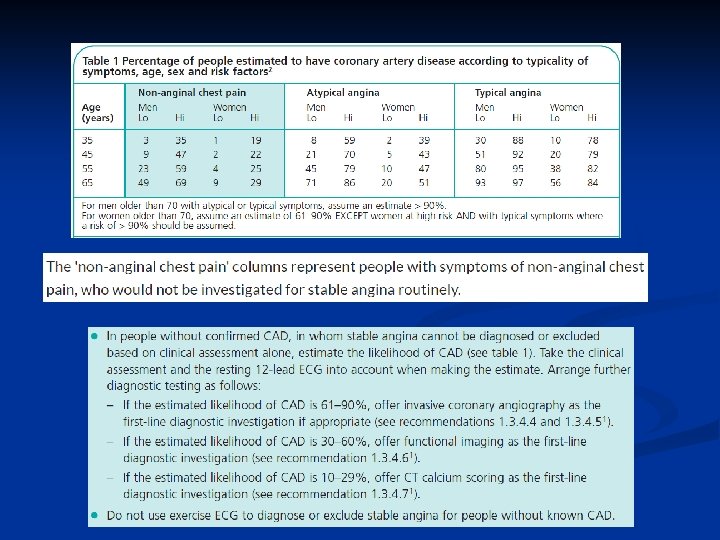
NICE Risk Prediction Charts overestimate presence of significant coronary artery disease

men women
 12 th July 2016 – ECTC Audit Day")
CT Coronary Angiography (CTCA) 12 th July 2016 – ECTC Audit Day

Treatment ? ?

Collateralized main stem occlusion

History of Treatment for Coronary Artery Disease Drugs 1867: Nitrates Propranolol Surgical Revascularisation PCI 1962: first LIMA-LAD 1967: saphenous vein grafts Nifedipine Atenolol 1960 1976: First balloon angioplasty 1980 1981: Captopril 1988: Aspirin (ISIS-2) Simvastatin Amlodipine Ticlopidine Clopidogrel 1986: first stent insertion 1990 Total arterial revascularisation Off-pump procedures Ivabradine Ranolazine Prasugrel, Ticagrelor, Vorapaxar Radial PCI 2000 2002: drug eluting stents Bioabsorbable stents 2010

The Value of Revascularisation

COURAGE Trial

BARI 2 D study

Diabetics are different! The FREEDOM trial

FREEDOM Outcomes at 2 and 5 years

What is the Extension of Survival with Coronary Artery Bypass Grafting?
 at 10 Years After CABG in Various Subgroups Overall")
Extension of Survival (in months) at 10 Years After CABG in Various Subgroups Overall Vessel disease One/two vessels Three vessels Left main LV function Normal Abnormal Exercise test Normal Abnormal Angina Class O, I, II Class III, IV VA risk score Low Moderate High Stepwise risk score Low Moderate High N=1300 N=150 N=550 Relevance today is unclear. There was minimal or no use of effective medical therapy (ASA, statins, beta-blockers, ACE inhibitors). Subgroup conclusions are based on pooling of predominantly negative trials. Extension of survival (mo) Yusuf et al. Lancet 1994; 344: 563 -570.

Is the Extent of Ischaemia still relevant in Times of Optimal Medical Treatment?

The more ischaemic myocardium, the more benefit from revascularisation-still true?

ISCHEMIA trial, are pills as good as revascularisation? Stable Patient Moderate or Severe Ischemia Blinded CCTA Core lab anatomy eligible? yes RANDOMIZE INVASIVE Strategy OMT + Cath + Optimal Revascularization no Late screen failure CONSERVATIVE Strategy OMT alone Cath reserved for OMT failures Average 4 Years of Follow-up Primary Endpoint: Composite of CV Death and MI

Some Case Studies

Mrs Gladys P, 84 years old Chest tightness and shortness of breath on exertion n Ex-smoker (40 py) with cholesterol 7. 4 mmol/l, HDL 1. 1 mmol/l, BP 120/80 mm. Hg, P 100 bpm n Creatinine 108 umol/l, TSH normal, Hb 89 g/dl, MCV 78 fl n On Ramipril 5 mg, Aspirin 75 mg OD n Normal resting ECG n

Mr Peter P, 64 years old Chest tightness on exertion n Hypertensive, cholesterol 6. 2, HDL 0. 8 mmol/l, diabetic n On Metformin 1000 mg BD, Ramipril 5 mg OD n Hb. A 1 c 75 mmol/mol n BP 160/90 mm. Hg, Pulse 75 bpm n

Mrs Pauline P, 68 years Chest tightness on exertion n Asthmatic, on Montelukast, Seretide, Tiotropium bromide n Positive FH for premature CAD n Hypercholesterolaemic n BP 140/90 mm. Hg, P 90 bpm n Phobia of needles n

Paul H, 48 years Stabbing chest pains, lasting seconds, not related to exertion n High cholesterol (7. 8 mmol/l, HDL 0. 8 mmol/l) n Positive family history for premature CAD n smokes n Worried! n

Thank you!
- Slides: 51