Invasive blood pressure monitoring in critical care Presented

Invasive blood pressure monitoring in critical care Presented by Ri 施易青

Outline n n n Introduction Arterial pressure waveform Controversial aspect of IBP monitoring Conditions that affect arterial waveform morphology Pros and cons of various cannulation sites
 First")
History n n n First invasive blood pressure monitoring: Stephen Hales’ horse (1733) First attempt in human: Faivre’s amputee (1856) Clinical use: Lambert and Wood (1947) Modern cannulation technique: Barr (1961) CV surgery in the 60 s

Indications n n n Continuous monitoring of BP Serial external monitoring inadequate Hypotension or hypertension requiring vasoactive drugs Respiratory illness or mechanical ventilation requiring frequent blood gases: >3 X/D for arterial sticks >5 X/D for combined arterial and/or venous sticks Major Surgery: Especially CV or neuro. procedures

Contraindications n n n n Absence of collateral flow Raynaud's disease and cold infusions Angiopathy, coagulopathy (recent anti-coag. or thrombolytic infusion increases risk of hematoma and compressive neuropathy), atherosclerosis: Use Caution! Avoid locating near A-V fistula, and inserting through synthetic graft Diabetics at increased risk of complications Avoid local infection, burn or traumatic sites Avoid extremities with carpal tunnel syndrome

: early systole, opening")
The Pressure-pulse n n n 1 st shoulder (the Inotropic Component): early systole, opening of aortic valve, transfer of energy from contracting LV to aorta 2 nd shoulder (the Volume Displacement Component): produced by continuous ejection of stroke volume from LV, displacement of blood, and distention of the arterial wall Diastole: when the rate of peripheral runoff exceeds volume input to the arterial circulation

Possible Information gained from a pressure waveform n n n Systolic, diastolic, and mean pressure Myocardial contractility (d. P/dt) Peripheral vascular resistance (slope of diastolic runoff) Stroke volume (area under the pulse pressure curve) Cardiac output (SV x HR)

Is arterial waveform predictive of cardiac contractility? n It is only “aortic arch pressure” that can be used to measure LV contractility, not “peripheral pressure”
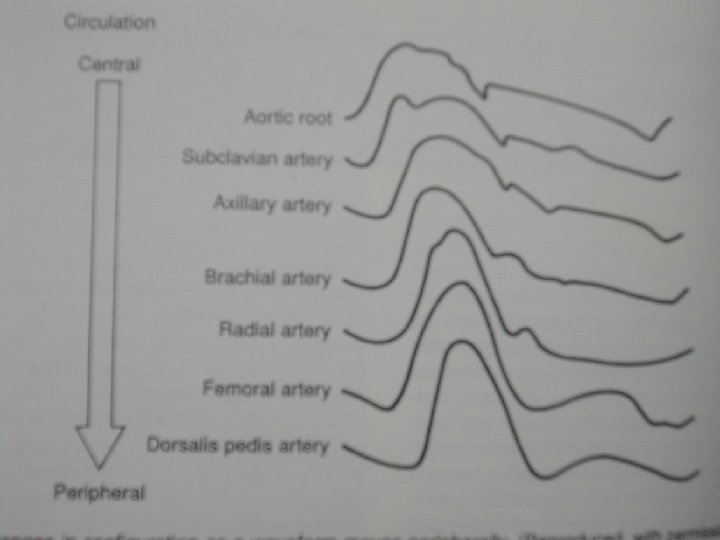

As BP is measured farther into periphery: n n n The anacrotic and dicrotic notches disappear The waveform appears narrower The systolic and pulse pressure increase The upstroke becomes steeper The diastolic and mean pressure decrease

Morphology changes as a result of peripheral reflexions: n n n Reflexion of waves due to the tapering diameter Reflexion due to changing content of the arterial wall Reflexion also occur at branching points of vessels

Is the arterial waveform predictive of stroke volume? n n n The pressure does not predict flow The distensible aortic arch act as a “fixed-capacity, high pressure reservoir” Flow in the arterial tree is continuous, with 10 -20 percent of LV power being pulsitile

n Cullen et al: Correlation coefficient of 0. 82 between changes in stroke volume and changes in peripheral systolic pressure in halothaneinduced anesthesia status, where peripheral vascular resistance remained essentially unchanged Interpretation of blood pressure measurement in anesthesia Anesthesiology, 40: 6 1974

Role of direct arterial pressure monitoring n n Provides trends over a wide range Unreliable as absolute hemodynamic values As a reminder “A needle in an artery does not guarantee a pressure or accuracy any more than an endotracheal tube guarantee a patent airway. ”

Conditions that affect arterial waveform morphology Hyperdynamic pulse n Pulsus paradoxus Reverse pulsus paradoxus n Pulsus alternans n Pulsus bisferens n n

Hyperdynamic pulse n n n Aortic regurgitation AV fistula Thyrotoxicosis Anemia Pregnancy sepsis

Pulsus paradoxus

Cause of pulsus paradoxus n n Change in pleural pressure associated with breathing Anatomic relationship between two ventricle chambers

D/D of Pulsus paradoxus n n Constrictive pericarditis or cardiac tamponade COPD Asthma Tension pneumothorax

Reverse pulsus paradoxus n n An exaggeration of the rise in systolic BP during mechanical ventilation A sensitive indicator of hypovolemia in mechanically ventilated p’t

Pulsus alternans

Cause of pulsus alternans n n A sign of decreased myocardial contractility (deletion of the number of myocardial cells contracting on alternate beats) An alteration in diastolic volume leading to beat-to-beat variation in preload

D/D of pulsus alternans n n LV dysfunction Pericardial effusion

Pulsus bisferens

Pulsus bisferens n n Hypertrophic cardiomyopathy Aortic regurgitation

Advantages and disadvantages on various cannulation sites Radial n Brachial n Femoral n Axillary Dorsalis pedis n n artery artery

Radial artery n n Advantages: easy to cannulate, accessible during most type of surgery, good collateral circulation, patient comfort, Allen’s test Disadvantages: thormbus formation, possible injury to nerve, augmentation of SBP,

Brachial artery n n Advantages: easy to cannulate, larger catheter, less SBP augmentation, collateral vessels Disadvantage: uncomfortable for p’t, median nerve damage

Femoral artery n n Advantages: prolonged use, useful in shock p’t, largest catheter Disadvantages: atherosclerotic plaque may break off, massive hematoma, difficult to immobilize

Axillary artery n n Advantages: large size, useful in peripheral artery dz and shock, proximity to aorta, Disadvantages: neurologic complication, technically difficult

Dorsalis pedis artery n n Advantages: dual circulation Disadvantages: greatest SBP augmentation, thrombus formation, difficult to immobilize, impossible to walk

Take home message n n The arterial system functions as a damped, resonant, transmission line, transmitting various frequencies with different degrees of attenuation. The clinician must dissuade himself from the belief that the peripheral pressure accurately reflects aortic arch pressure.

reference n n n Monitoring in Anesthesia and Critical Care Medicine, 2 nd edition. 1990 Hemodynamic monitoring: Invasive and Noninvasive Clinical application, 2 nd edition. 1995 Cullen et al: Interpretation of blood pressure measurement in anesthesia. Anesthesiology, 40: 6 1974

Thanks for your attention!
- Slides: 35