Intussusception Introduction l l The most common abdominal

Intussusception

Introduction l l The most common abdominal emergency in early childhood, particularly in children younger than two years of age, and the second most common cause of intestinal obstruction after pyloric stenosis. Intussusception is unusual in adults, and the diagnosis is commonly overlooked. In the majority of cases in adults, a pathologic cause is identified. In contrast, the majority of cases in children are idiopathic.
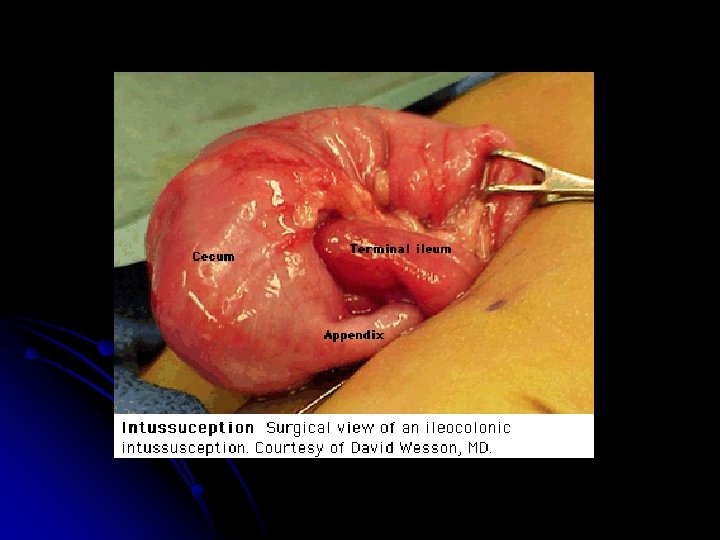
 Most common: ileo-colic type others: ileo-colic, jejuno-jejunal, jejuno -ileal, or colo-colic")
Pathogenesis (2 -1) Most common: ileo-colic type others: ileo-colic, jejuno-jejunal, jejuno -ileal, or colo-colic intussusception l Intussusception is considered to be idiopathic (ie, no lead point can be identified) in more than 75 percent of children with ileo-colic intussusception. l
 A lead point is recognized more commonly in children >5")
Pathogenesis l (2 -2) A lead point is recognized more commonly in children >5 y/o. A variety of pathologic conditions associated with intussusception, including: small bowel lymphoma Meckel diverticulum duplication cysts polyps vascular malformations inverted appendiceal stumps parasites (eg, Ascaris lumbricoides) Henoch-Schönlein purpura
 Approximately 60 percent of children are younger than one year")
Clinical Manifestation (3 -1) Approximately 60 percent of children are younger than one year old, and 80 percent are younger than two. l Patients typically develop the sudden onset of intermittent, severe, crampy, progressive abdominal pain, accompanied by inconsolable crying and drawing up of the legs toward the abdomen. l
 The episodes usually occur at 15 to")
Clinical Manifestation l l l (3 -2) The episodes usually occur at 15 to 20 minute intervals. They become more frequent and more severe. Vomiting may follow episodes of abdominal pain. Initially emesis is non-bilious, but it may become bilious as the obstruction progresses. Between the painful episodes, the child may behave relatively normally and be free of pain. As symptoms progress, increasing lethargy develops, which can be mistaken for meningoencephalitis.
 Classic triads: abdominal pain, a palpable sausage shaped abdominal mass,")
Clinical Manifestation (3 -3) Classic triads: abdominal pain, a palpable sausage shaped abdominal mass, and currant-jelly stool. l Less than 15% of patients at the time of presentation. l

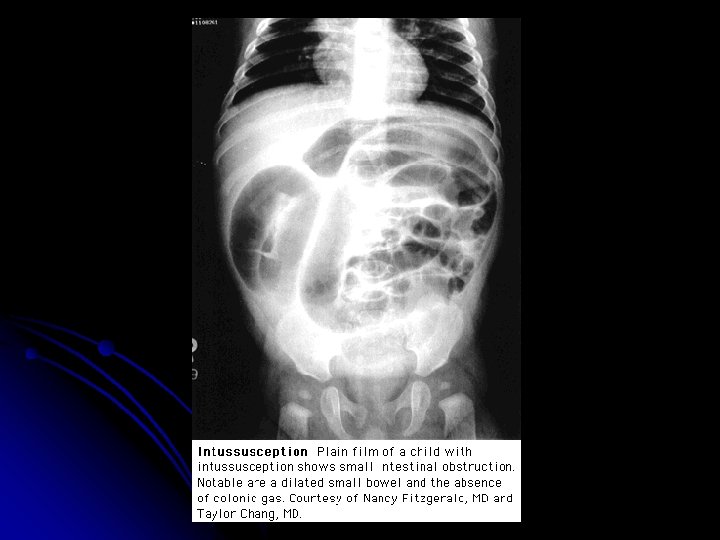
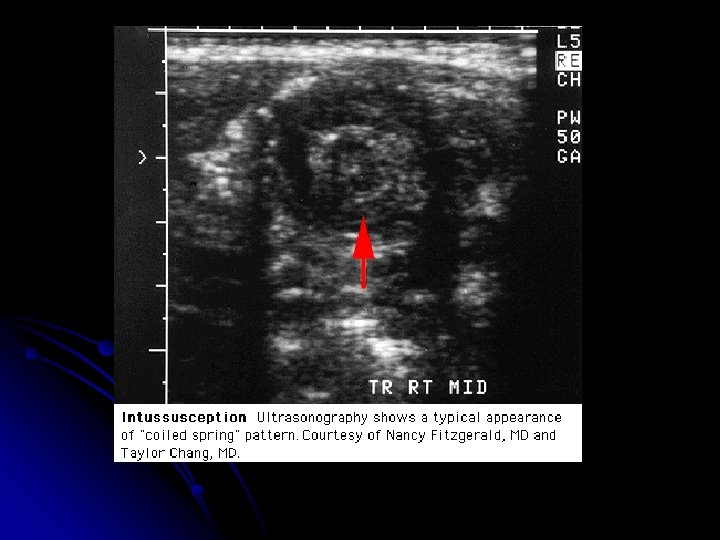
Diagnosis & Treatment l Abdominal plain films: l Crescent sign l Target sign l Ultrasonography: l Bull’s eye sign l Coiled spring sing l Target sign l CT scan (3 -1)

Crescent sign in LUQ.

Crescent sign: Note the intussusceptum lead point ascending into the hepatic flexure.

Intussusception Possible target sign in RUQ. Paucity of bowel gas suggestive of rightsided mass and bowel obstruction. X-ray diagnosis? 7 -month-old girl with skull fracture, lethargy, and vomiting.
 Contrast studies: l The standard procedure for diagnosis")
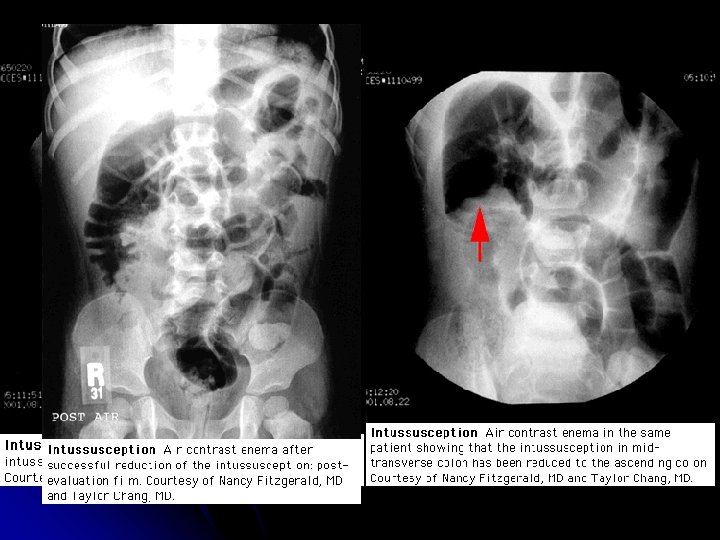
Diagnosis & Treatment l (3 -2) Contrast studies: l The standard procedure for diagnosis and treatment of intussusception is a contrast (air or radiopaque) enema. l Barium and water-soluble contrast l Air contrast l Nonoperative reduction using barium or air contrast techniques is successful in approximately in 75 to 90 percent of patients with ileo-colic intussusception.
 High risk cases: l symptoms longer than 48")
Diagnosis & Treatment l (3 -3) High risk cases: l symptoms longer than 48 hours l Infant < 1 y/o (esp. <3 m/o) l children > 5 y/o, and when plain films show signs of intestinal obstruction Recurrance rate: approximately 10% l Surgery l


- Slides: 19