Introduction to UK GO data GPRD General Practice

 • >6% of")






 • No")




")
")
 DM Non-DM")
 DM Non-DM Adjusted: age, sex, smoking, morbidity")
")
 by treatment")
 Met- Met+ Exposed anytime aft Ca. diag HR=0. 72; 0.")
- Slides: 21
Introduction to UK GO data GPRD: General Practice Research Database THIN: Health Improvement Network Some new data too
Data sources • Records from GP routine records • GPRD=THIN (almost) • >6% of the UK population • >350 GP practices • >6½ million individual people
UK NHS―National Health Service • Largest UK employer― 4 th largest employer in world • 1. 7 million employees • 40, 000 GPs • 10, 000 GP practices • GPs see 140 patients per week
Data content • Diagnoses: GP and some hospital • Biochemistry: Hb. A 1 c etc • Risk factors: weight, smoking etc • Family history (some) • Drugs (all prescribed drugs) • Outpatient contacts • Free text • GPRD only…. linked data: • Cancer registry data • Hospital inpatient data
Quality: representativeness
Quality: completeness
Quality: completeness
Strengths • Size―over 5% UK population • Nationally representative • Fast―information already collected • Frequent collections • All prescribable drugs • Population based • Study design flexibility • ‘Real Life’ data―collected during normal GP visit • Link to GP and patient for additional information
Weaknesses • £cost! • No direct link to secondary care data (THIN) • No direct link of prescriptions to diagnoses temporal implied link • Limited information on OTC medications • Limited data on lifestyles, diet etc • Not dispensed prescriptions • Limited information on hospital prescribing • Some medications only administered by specialists
Weaknesses re Ca. • Details of the cancer diagnosis variable • No systematic cancer staging data • Metastatic cancer: have to infer • Hospital cancer treatments not known
New data! Survival after incident cancer: diabetes vs. non-diabetes
Incident cancers by cancer site
Incident cancers by DM treatment
Mean survival by Ca. site (years)
Δ mean survival by Ca. site (years)
Cumulative mortality (crude) DM Non-DM
Cumulative mortality (adjusted) DM Non-DM Adjusted: age, sex, smoking, morbidity
HR DM vs-N-DM (Cox)
adj. HR: DM vs N-DM (=1) by treatment
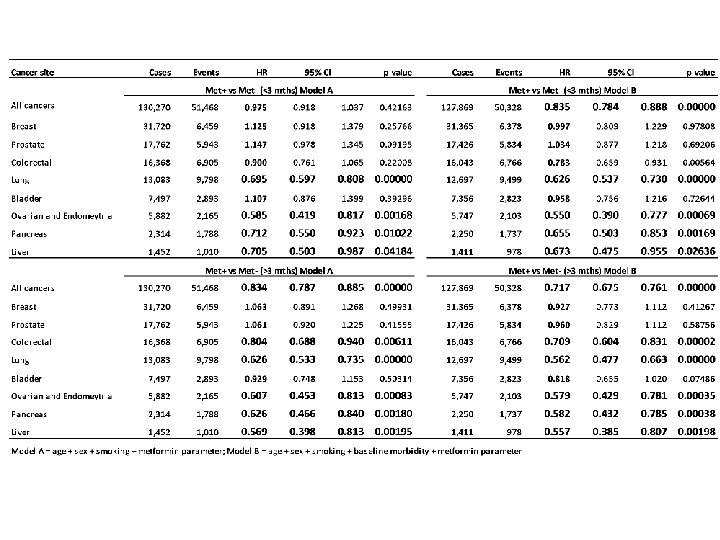
Cum-mortality: ± metformin (adjusted) Met- Met+ Exposed anytime aft Ca. diag HR=0. 72; 0. 68 -0. 76; p<0. 00001 Met+ Exposed in first 3 months HR=0. 83; 0. 78 -0. 89; p<0. 00001