Introduction to the Gastrointestinal System Summary n n






 Subcutaneous (fatty/adipose layer)")



 contents: liver gallbladder")
 contents: stomach spleen left lobe")
 contents: cecum appendix right ovary")
 contents: part of descending colon")



















 Neoplasm (benign")


 Chronic Pancreatitis Trauma")
")
 Cyst")





 Dye Antibiotic Irrigation Topical Hemostatics Local")
 MAC (IV Sedation with Local) Spinal")















 Cyst Lump (Benign")


 Minor tray Breast Retractors Extra hemostats Plastic")


 “Rule of 5’s” 5")











 n Rigid Visualization: Direct (0°) Angled (30, 70, 120°)")
 No operating channels Can be")











- Slides: 114
Introduction to the Gastrointestinal System
Summary n n n Anatomy & Physiology, Pathology and Operative Considerations for: GI System Breast IVAD Care & Use of Endoscopes
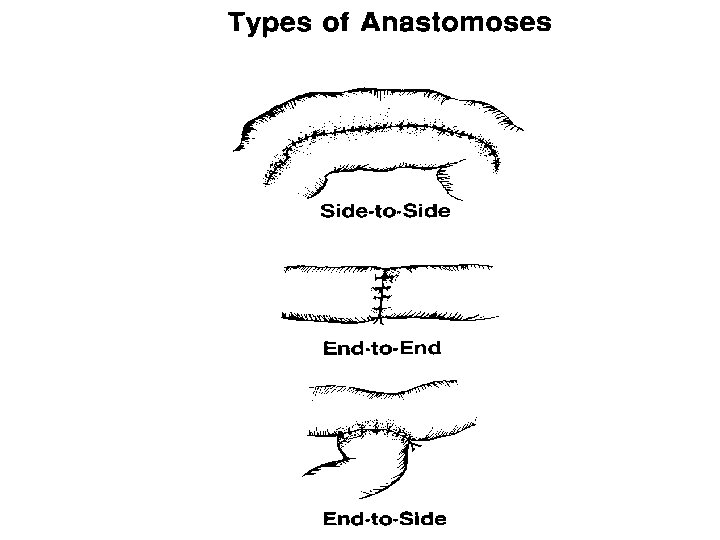
Gastrointestinal Definitions n n n n Adhesion- tissue that is normally separate is bound together; produced by inflammation, injury, or intentionally surgically created Anastomosis- joining of parts to create a union Bile- yellow-green alkaline fluid produced by the liver that aids in digestion and fat absorption Biliary tract- system of the body involved with bile production, secretion, and transport Cholangiogram- injection of contrast media into the cystic duct or a tube placed in the common bile duct to allow visualization of the biliary ductal system Cholecystitis- inflammation of the gallbladder Cholelithiasis- stones in the gallbladder Colon- large intestines
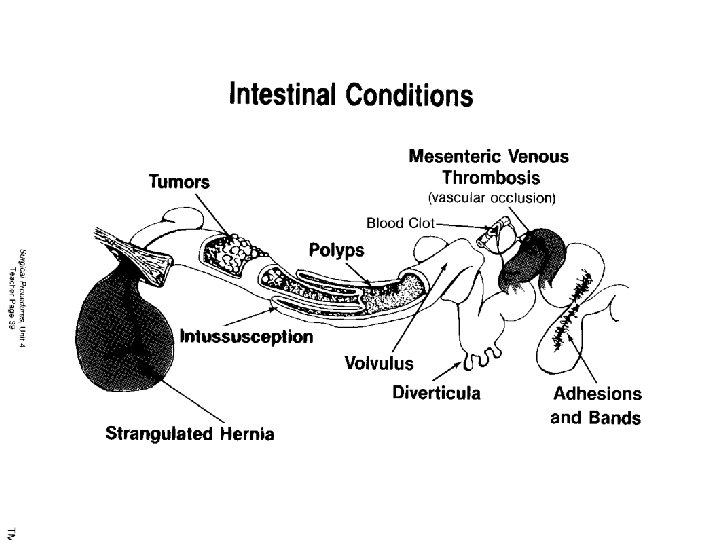
Gastrointestinal Definitions n n n n Diverticula- small pouches in the lining or wall of a canal or organ, most commonly the colon Dysphagia- difficulty swallowing Fissure- crack or opening Fistula- abnormal passage between two surfaces or two hollow organs Intussuseption- when part of the upper intestine slips into or invaginates into a lower portion of the intestine/creates an intestinal obstruction Meckel’s diverticulum- congenital blind pouch usually associated with the ileum and ileocecal valve Mucosa- mucous membrane
Gastrointestinal Definitions n n n n Peptic ulcer- open lesion in the stomach or duodenum Peritonitis- inflammation of the peritoneal cavity Polyp- growth or tumor with a stalk or pedicle extending from a mucous membrane Pyloric stenosis- congenital narrowing between the stomach and duodenum (pyloric orifice) due to thickening of circular muscle surrounding it Resection- excision of a structure and reconstruction of what remains Sphincter- ring-like muscle surrounding an orifice Volvulus- twisting or torsion of the intestine causes obstruction and possible strangulation
General Surgery n n n Abdominal Wall Abdominal Cavity Abdominal Organs Breast (excluding reconstructive procedures) Vascular Access (excluding dialysis shunting access procedures) Can include tracheotomy, thyroidectomy and parathyroidectomy
Anatomy of the Abdominal Wall n n n n Subcuticular (skin) Subcutaneous (fatty/adipose layer) Anterior fascia (thin or thick membrane over the muscle) Muscle Posterior fascia (thin or thick membrane under the muscle) Omentum (lesser and greater) Peritoneum (shiny membrane covering the abdominal cavity) Contents of abdominal cavity (organs/viscera)
Abdominal Cavity n n Diaphragm to pelvic base Pelvic girdle Ribs Vertebrae
Abdominal Surgery Landmarks n n n n Xiphoid process Subcostals Iliac crests Symphysis pubis Umbilicus Linea alba Serve as reference points for incisions and internal organ access
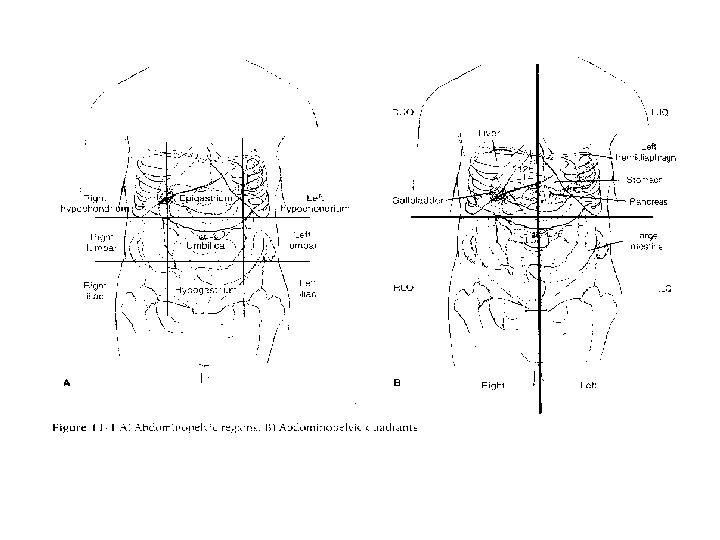
Abdominal Divisions n n Four Quadrants Nine Quadrants
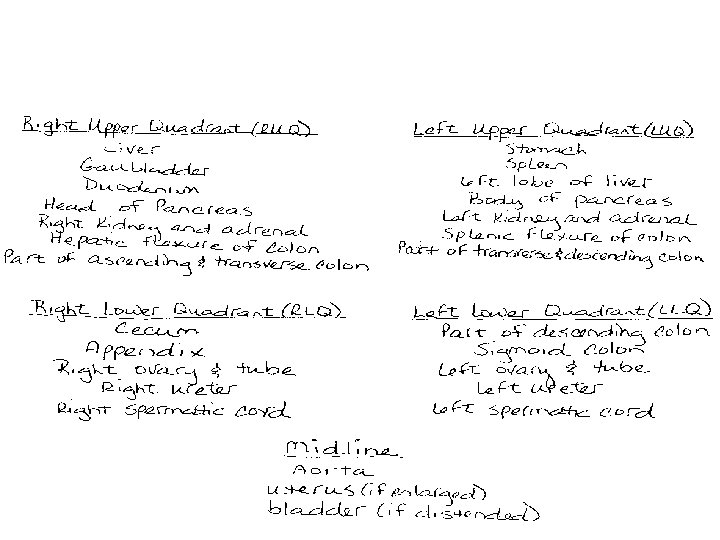
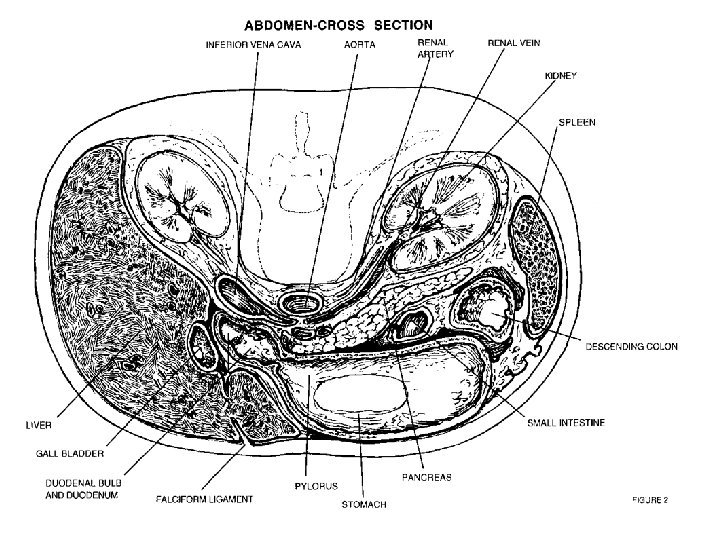
Abdominal Division n Anatomy of the Abdomen RUQ (right upper quadrant) contents: liver gallbladder duodenum head of pancreas right kidney and adrenal part of ascending and transverse colon
Anatomy of Abdomen Continued n LUQ (left upper quadrant) contents: stomach spleen left lobe of liver body of pancreas left kidney and adrenal part of transverse and descending colon
Anatomy of Abdomen Continued n RLQ (right lower quadrant) contents: cecum appendix right ovary and fallopian tube right ureter right spermatic cord
Anatomy of Abdomen Continued n LLQ (left lower quadrant) contents: part of descending colon sigmoid colon left ovary and fallopian tube left ureter left spermatic cord
Anatomy of Abdomen Continued n Midline of Abdomen: Aorta Uterus Bladder
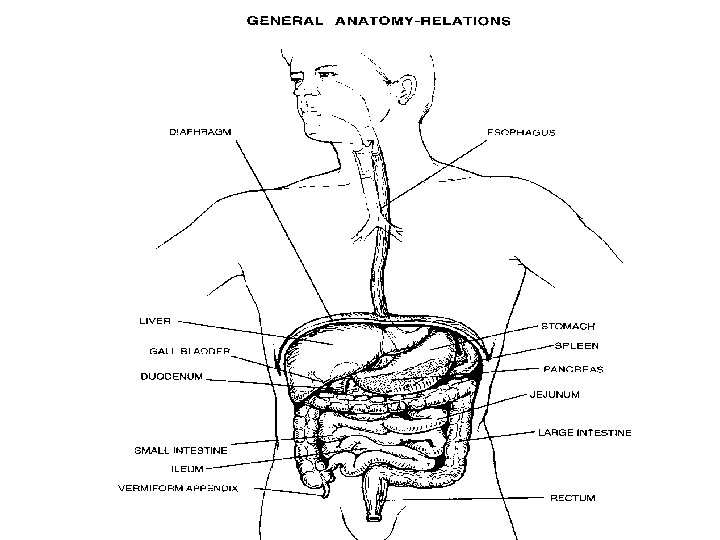
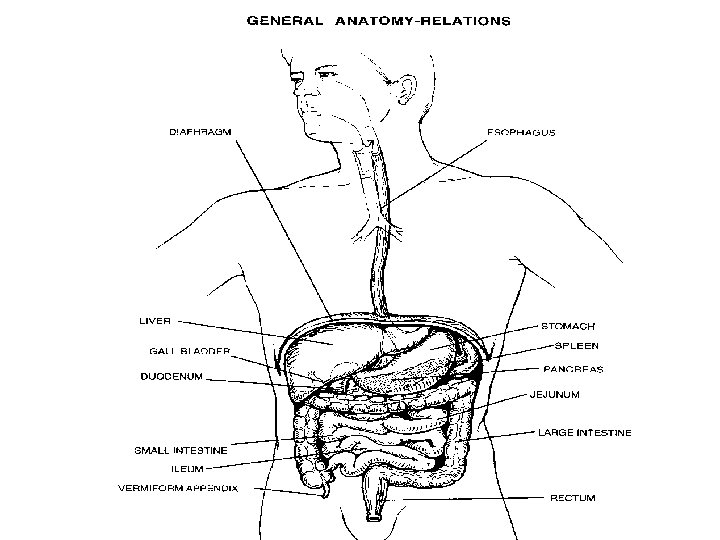
Digestive Tract Alimentary Canal n n Mouth to the Anus Mouth>Pharynx>Pharyngoesophageal Sphincter>Esophagus> Esophagogastric Sphincter>Stomach>Pyloric Sphincter >Duodenum>Jejunum>Ileum>Cecum (appendix)>Ascending Colon>Transverse Colon>Descending Colon>Sigmoid Colon>Rectum>Internal Sphincter>External Sphincter>Anus
Physiology of the Digestive System n n n Two major parts: GI tract/alimentary Canal -mouth to anus -about 30 ft long Accessory Organs -outside of or to side of GI tract, but are connected -teeth, salivary glands, biliary system: liver, gallbladder, pancreas
Physiology of the Digestive System n n n 5 major processes: Ingestion/eating Mechanical and Chemical Digestion Peristalsis Absorption Defecation
Mechanical and Chemical Digestion n Begins in mouth, teeth increases surface area of food to allow enzymes to work on Tongue pushes food underneath teeth and flips food as a “bolus” to back of throat (oropharynx) Salivary Glands-primary salivary amylase begins break down of carbohydrates
Mechanical and Chemical Digestion n Esophagus: Begins at oropharynx Mucous allows food to slide down
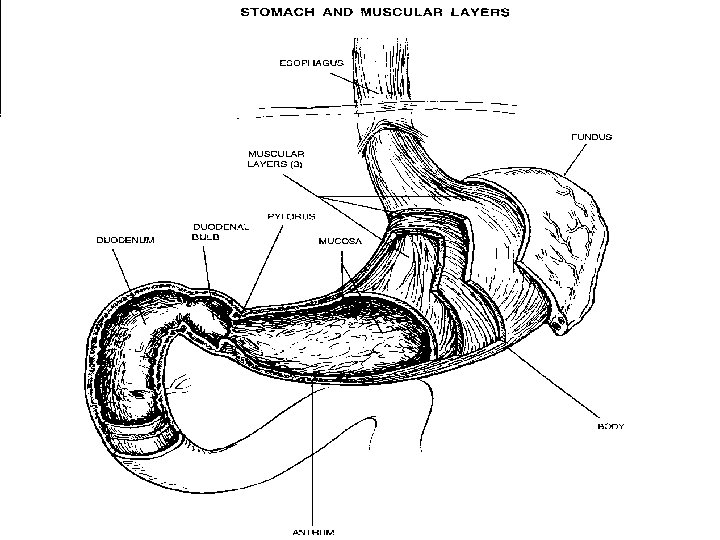
Mechanical and Chemical Digestion n n 1. 2. 3. 4. Stomach 4 areas: Cardiac (esophagus ends and cardiac or esophageal sphincter empties into this region Fundus/fundic area part that is rounded on left side of body Body-main part of stomach Pyloric region or antrum=area before pyloric sphincter which is where the duodenum begins
Mechanical and Chemical Digestion n n 1. 2. 3. n n n Rugae (hills and valleys allow stomach to expand 3 basic cell types here that produce: Pepsinogen HCl Mucous HCl acid activates pepsinogen which then becomes pepsin which begins protein breakdown Vagus nerve stimulates tunica muscularis to create waves in stomach from bottom up to allow for mixing of HCl and pepsin Vagus nerve tires easily, production of hormone gastrin by the stomach sustains the action of stomach wave action Food in stomach 1 -6 hours Food broken down into “chyme” (semi-solid or pasty material
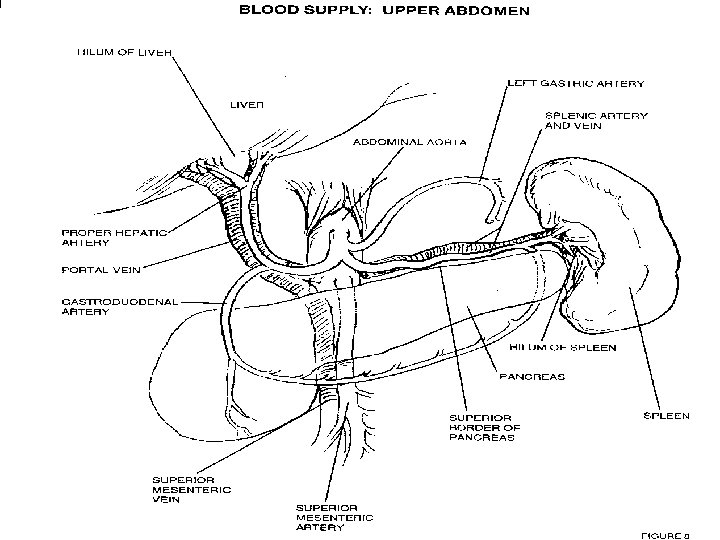
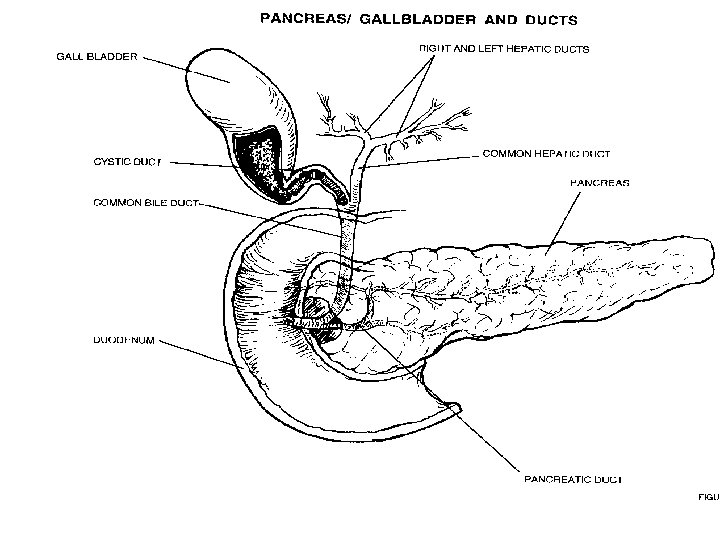
Pancreas n n n Head Body Tail 80% comprised of lobules Lobules consist of exocrine and endocrine glands
Mechanical and Chemical Digestion Pancreas n Endocrine and exocrine gland 1. Endocrine portion = Islets of Langerhan n No ducts, secrete into blood or lymph n Secreting portion is Islets of Langerhans n 1% of pancreatic mass n Receives 25% pancreatic blood supply n
Islets of Langerhan n n Two cell types: Alpha cells secrete hormone glucagon (↑ blood sugar level) Beta cells secrete hormone insulin (↓ blood sugar levels) Function maintenance of blood glucose levels
Exocrine glands n n Secrete directly through a duct Called acini Functions: breakdown fats, proteins, carbohydates and maintain p. H maintenance prevents excessive acid production which prevents duodenal ulcers
Mechanical and Chemical Digestion Pancreas 2. Exocrine portion: 1. Produces enzymes: collectively called pancreatic juices (Trypsin, chymotrysin, carboxypeptidase) break down proteins 2. Pancreatic amylase breaks down carbohydrates 3. Pancreatic lipase breaks down lipids n All get to small intestine via pancreatic duct (Duct of Wirsung) at Ampula of Vater n
Mechanical and Chemical Digestion n n Liver Functions: Store excessive nutrients Detoxify and filter toxins Regulate nutrient levels Destroy worn out RBCs, WBCs, bacteria Produce heparin, prothrombin, fibrinogen, and albumin Store fat soluable vitamins (A, D, E, K) Water soluable are excreted Produces bile (function to emulsify lipids)
Mechanical and Chemical Digestion n Gallbladder Stores bile Sphincter of Oddi opens to release bile into small intestine when lipids are present, otherwise remains closed
Mechanical and Chemical Digestion n n n 1. 2. 3. Small Intestine Begins at pyloric sphincter, ends at ileocecal valve About 21 feet long Where 90% of digestion and absorption occur Other 10% in stomach and large intestines 3 parts: Duodenum-(12 inches long) Jejunum (8 feet long) Ileum (12 feet long)
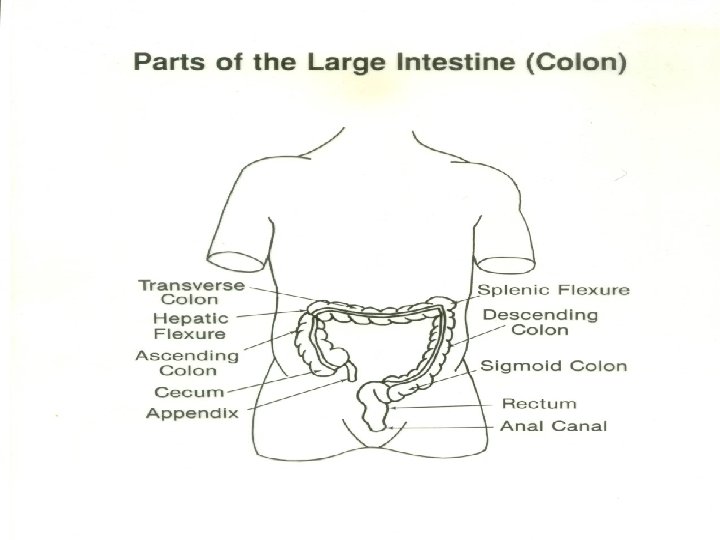
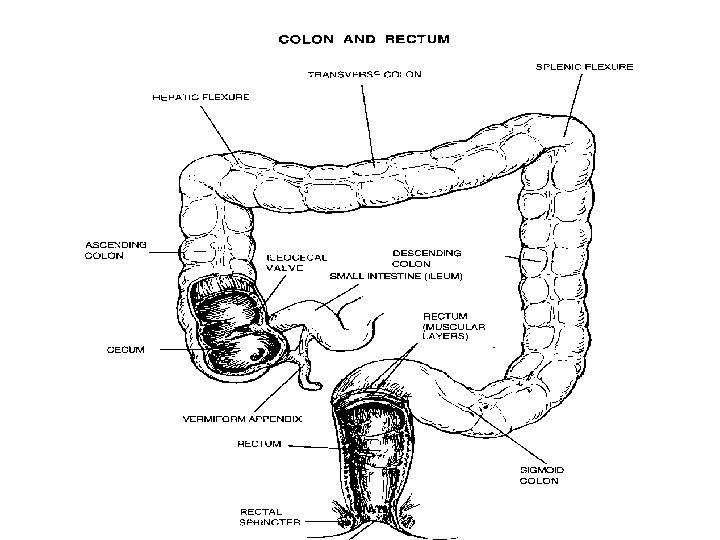
Mechanical and Chemical Digestion n n n Large intestine Parts of: Ascending, transverse, descending, sigmoid, rectum Functions: Absorption of water, electrolytes, proteins into amino acids, and bacterial products Feces formation Food in large intestine 3 -10 hours for absorption purposes Undigested food is expelled via “mass peristaltic movement” out the anus
Pathology of The Stomach n n n Ulcers Gastritis Polyps Bezoar (hairball in animals/fiber ball in humans) Carcinoma Lymphoma (benign or malignant)
Small Intestine n n n Duodenum Jejunum Ileum
Pathology of the Small Intestine n n Ulcer (duodenum most common site) Neoplasm (benign or malignant) Obstruction Crohn’s Disease (Surgical intervention needed with perforation, abscess or hemorrhagic fistula formation)
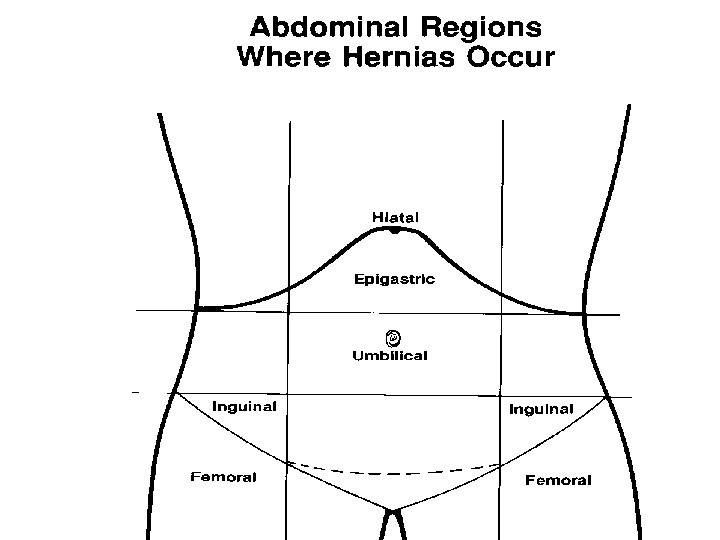
Colon Pathology n n n Appendicitis Adhesions Herniation Polyps Diverticulosis or Diverticulitis Tumor (benign or malignant) Ulcerative Colitis Obstruction Volvulus Intussusception Impaction
Anorectal Pathology n n Fistula Fissure Pilonidal Cyst Hemorrhoids
Pathology of the Pancreas n n Cyst Tumor (Benign or Malignant) Chronic Pancreatitis Trauma
Spleen n n Largest lymphatic mass in body Composed of: 75% red pulp (vascular) 25% white pulp (lymphatic/immune response) Functions: RBC and Plt storage Excision of renders liver and other lymphatic tissues to pick up the slack
Pathology of the Spleen n n Trauma Hematologic Disorders Tumor (Benign or Malignant) Cyst Splenomegaly
Liver Largest organ in the body n Comprised of 4 lobes n Functions: *Bile production *Metabolism of fats, proteins and carbohydrates *Glycogen storage *Storage of fat soluable vitamins (A, D, E, K) and Fe, Cu *Detoxification *Prothrombin and fibrinogen synthesis n
Pathology of the Liver n n n Carcinoma Trauma FYI: Cirrhosis is related to hepatic cancer Cirrhosis results from hepatitis and chronic alcohol abuse
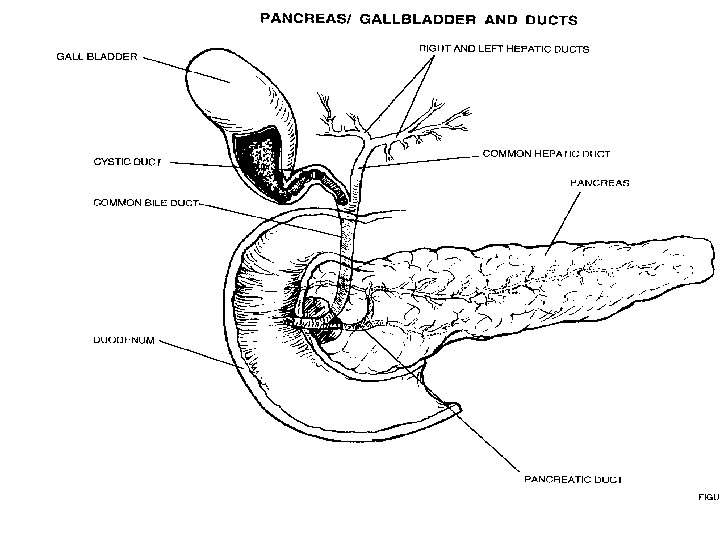
Biliary Tract n n n n Gallbladder, cystic duct, common bile duct, and common hepatic duct Function: transport bile, store bile and release bile into the duodenum Aids in digestion and absorption of fats Gallbladder divided into fundus, body and Hartman’s pouch: most common site of gallstones (clog and prevent passage of bile into cystic duct) Sphincter of Oddi: where CBD empties into duodenum/controls release of bile into duodenum Ampulla or papilla of Vater is an enlarged area where the duodenum joins CBD
Biliary Pathology n n n Acute Cholecystitis Cholelithiasis Chronic Cholecystitis Gallbladder calcification Tumor (benign or malignant)
Pre-Operative Testing & Diagnosis n n n n n Family History Symptomatic Liver Function Blood Tests Pancreatic Function Blood Tests Barium Studies Endoscopic Studies (Visualization, Biopsy, ERCP with C-Arm) Ultrasound CT Scan MRI
Medications n n n Contrast Media (Hypaque) Dye Antibiotic Irrigation Topical Hemostatics Local
Anesthesia n n n General MAC (IV Sedation) MAC (IV Sedation with Local) Spinal Epidural Local
Instrumentation n n n n Minor tray Major Tray Intestinal Tray Gallbladder Tray Laparoscopic Accessories Extra Long Instrument Tray Scopes
Equipment n n n X-Ray Table Laparotomy Endoscopic Tower (video monitor, insufflation tubing, insufflator, light cord, light source, camera box, camera, scope warmer)
Supplies n n n n n Laparotomy Pack Basic Pack Laparotomy Sheet Universal Sheet Minor Basin Set Suture of Surgeon choice Kittners Gloves Blades Cholangiogram Supplies (Sterile specimen cup, stopcock, IV tubing, 30 cc syringes x 2)
Positioning n n n Supine trendelenburg reverse trendelenberg Kraske Lateral
Prepping n n n Betadine Scrub Betadine Paint Duraprep Alcohol Hibiclens Surgeon Preference
Draping n n n Towels Stapler or towel clips Optional Ioban or Vi-Drape Laparotomy Sheet Universal Sheet Surgeon Preference
Procedure for Opening Abdominal Cavity n n n n Skin incised Blood vessels cauterized Fascia incised Muscle layers divided or separated Fascia incised Omentum displaced (intestinal bag prn) Peritoneum incised Abdominal cavity contents exposed
Abdominal Incision Type Considerations n n n Surgeon selects incision that will best expose the structure to be operated on Surgeon selects incision that will create minimal trauma and post-operative pain Surgeon selects incision that will allow for wound closure strength as closed by primary wound healing
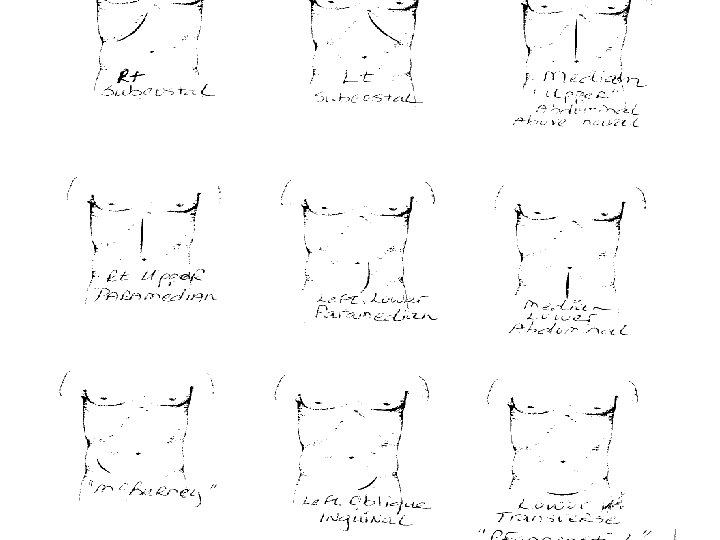
Abdominal Incision Types n n Right Subcostal gallbladder, biliary system Left Subcostal spleen Median Upper Abdominal stomach, duodenum, pancreas Median Lower Abdominal uterus, adnexa (ovaries, fallopian tubes), bladder
Abdominal Incision Types n n n Right Upper Paramedian stomach, duodenum, pancreas Left Lower Paramedian pelvic structures, colon Mc. Burney appendix Left Oblique Inguinal hernia repair Lower Transverse (Pfannensteil) uterus, ovaries, and fallopian tubes
Dressings n n n Packing prn 4 x 4 s ABD Pad Tape Will vary with Surgeon and Procedure
Drains n n n Penrose Jackson Pratt Snyder Blake May use grenades or hemovac Varies with Surgeon Preference and Procedure
Postoperative Care & Considerations n n n PACU or ICU Minor procedures may D/C to home Possible complications: hemorrhage, infection, recurrence of pathology, bowel obstruction, wound dehiscence or evisceration, atelectasis>pneumonia,
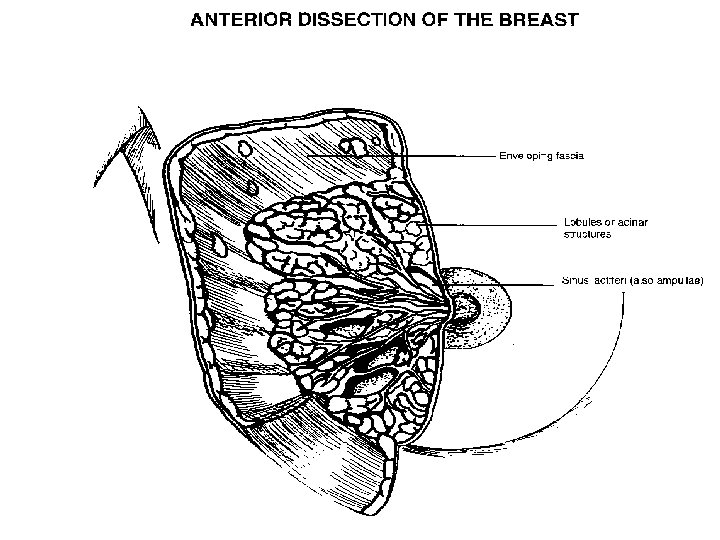
The Breast
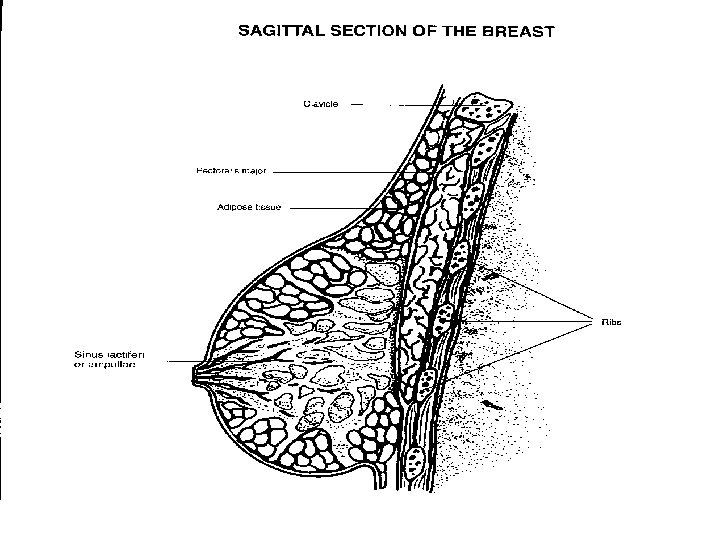
Anatomy of the Breast n n n n Mammary Gland Modified Sweat Glands Anterior to the Pectoralis Major Muscle 15 to 20 lobes Reproductive System (accessory) Secrete milk for infant Functionless in the male Well vascularized
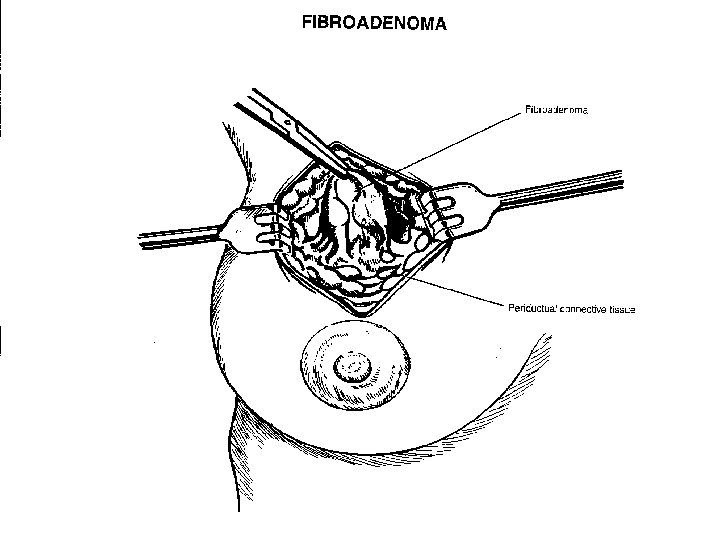
Pathology of the Breast n n n Abscess Fibroadenoma (benign lesion) Cyst Lump (Benign or Malignant) Mass/Tumor (Benign or Malignant)
Diagnosis R/T Breast n n n Self-Breast Exam Mammogram Ultrasound Chest X-ray Bone Scan
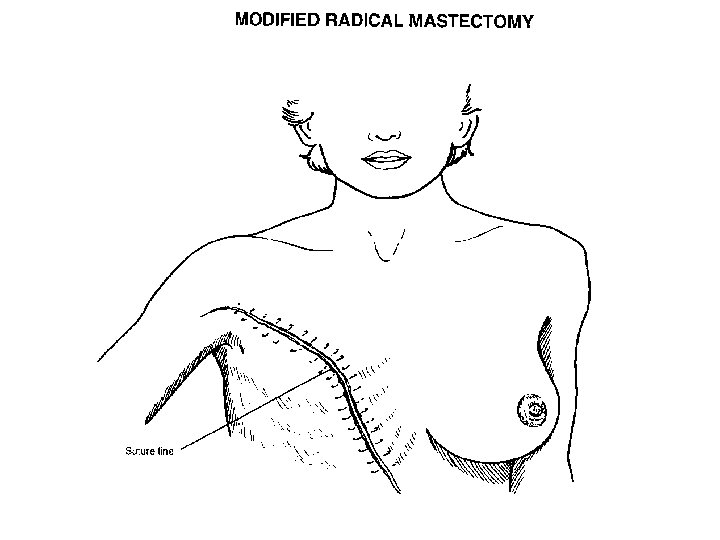
Surgical Breast Procedures n n n Biopsy Lumpectomy Segmental Resection Simple Mastectomy (preservation of pectoralis muscles and axillary nodes) *Modified Radical Mastectomy (preservation of pectoralis muscles) Radical Mastectomy
Equipment/Instruments/ Supplies n n n Routine (armboards) Minor tray Breast Retractors Extra hemostats Plastic Tray (prn) Laparotomy pack Minor basin set Suture of surgeon choice Blades Gloves Dressing Drain of surgeon choice
Medications & Anesthesia n n n Local Antibiotic irrigation Dyes: Marking pen Isosulfan Blue (Vital Blue) Technetium Biopsies will be done under Local General with local anesthesia
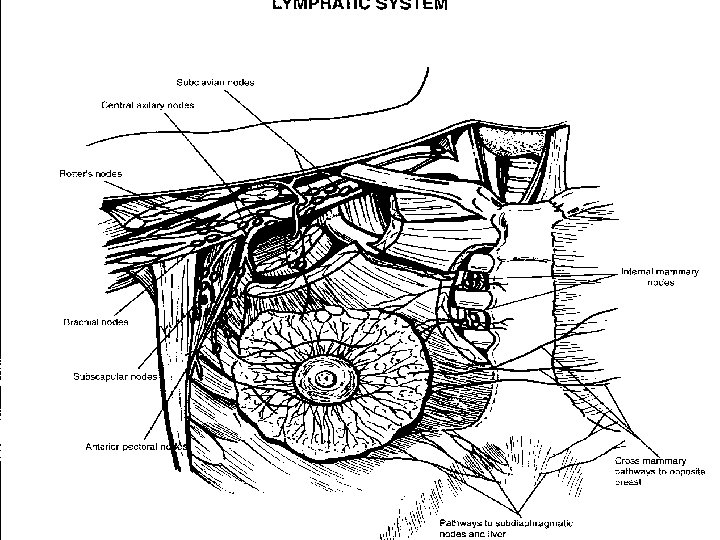
Sentinel Nodes n n May hear or see “Sentinel node” associated with a breast procedure This just refers to the first lymph nodes along the lymphatic channel from where the tumor originates Not in the same place in every patient Helpful in determining extensiveness of malignancy
Sentinel Node Biopsy n n n Isosulfan Blue (Vital Blue) “Rule of 5’s” 5 ml, 5 cm area, 5 sites, 5 minute massage Remove blue stained nodes Await pathology results May involve further breast or axillary dissection
Sentinel Node Biopsy n n n n Technetium Injected in nuclear medicine department Is radioactive material “Rule of 6’s” 6 ml, 6 sites, 6 cm area, 6 minute massage prior to exploration of nodes Wand passed over that detects “hot” areas Surgeon will mark site with a marking pen and proceed with dissection of nodes or further intervention
Positioning n n Supine Affected arm on armboard
Prep n n n Performed extensive in event need to extend excision Anterior chest from neck to umbilicus, upper affected arm to affected axilla Prep should be gentle particularly if open breast biopsy with needle (wire) localization in place
Draping n n Laparotomy sheet or universal drape May use split sheet for affected arm
Dressing/ Drains/Post-op Care n n n Fluffy dressing Drains of surgeon choice PACU Post-operative complications: Hematoma, hemorrhage, infection, cellulitis, impaired arm movement, anesthesia of anterior chest wall Chemotherapy and/or Radiation
Vascular Access Procedures
Vascular Access Procedures n n n Cannulation of arteries and veins General surgeons primarily will do venous access procedures (IVAD) Performed percutaneous or via cut-down Indicated for chemotherapy, nutrition (TPN), blood product infusion, needle phobia, pediatric patients, CVP monitoring needed, exhausted peripheral venous access) Types: Broviac, Groshong, Hickman, and Port-A-Cath
Complications of IVAD Insertion n n Thrombosis Infection Nerve Damage Pneumothorax Hemorrhage due to inadvertent arterial puncture
Dressing/Postoperative Care n n n n Prior to placing port caps on lumens need to flush ports with 1. 5 ml to 3 ml of Heparin 5, 000 ut per ml or heparin mixture of surgeon choice (refer to package insert) Betadine or Neosporin ointment on site where catheter penetrates skin (surgeon preference 2 x 2 (surgeon preference) Tegaderm of appropriate size Surgeon may want you to cover patient with sterile drape until chest x-ray performed to verify placement and intactness of pleura around lungs If not, do not breakdown table until line placement verified Carefully remove drapes so as not to dislodge catheter (place a towel over entire area prior to drape removal)
CARE & HANDLING OF ENDOSCOPES
Endoscopes Diagnostic 2. Operative (channeled) n Rigid Visualization: Direct (0°) Angled (30, 70, 120°) n Semi-rigid n Flexible Visualization: Panoramic 1. Two Types of Flexible: 1. Fiberoptic Visualization through eyepiece Connect to light source 2. Videoscope Visualization on monitor Connect to light source and camera
Diagnostic Endoscopes n n n Diagnostic purposes (looking around) No operating channels Can be used if more than one port will be utilized (cholecystectomy, thoracoscopy, etc. ) for visualization during utilization of other laparoscopic instrumentation for operative puposes
Operative Endoscopes n n n Channeled: irrigation, suction, insertion of biopsy forcep or needle, connection of accessory instruments such as cautery or laser Normally involves one port access (cystoscopy) Can always use another port
Use & Care of Endoscopes n n n Light Cords/Source Incandescent first used Problem: patient tissue damage due to the intense heat that was transferred through the light source and cord
Use & Care of Endoscopes n n n Light Cords/Source Fiberoptics used today “Cold Light” Heat is not transferred through the scope No patient tissue damage
Use & Care of Endoscopes n n n n Light Cords/Source Cord ends DO get HOT Light source should be off prior to connection and disconnection from the scope Avoid looking into light beam from light source or cord Light cords may not have universal fitting Are adaptors Light cords usually specifically made to fit the scope Do not bend cord/coil loosely due to multiple glass fragments (hence fiber optics) contained in the cord
Use & Care of Endoscopes n n n Scopes Should keep scope in a scope warmer until ready to use on the field to avoid fogging of the scope as a cold scope passing into a warm patient’s body WILL fog DO NOT place “Operative Scopes” in a scope warmer Avoid bending the scope where eye piece attaches to scope itself (If loose have poor visibility) Avoid slamming or scratching the scope
Use & Care of Endoscopes n n n Connection of scope, camera, light cord = “White Balancing” Prior to passing to surgeon for use must white balance the scope Cannot do this until all parts are connected and all tower sources are turned on Allowance of camera to pick up white so it will be able to differentiate primary colors for optimal visualization Hold scope close to a white sponge, lap, towel May be done on the field by pressing balance button on newer cameras or by the circulator pressing the balance button on the camera box
Use & Care of Endoscopes n n n Cleaning: Keep endoscopic instruments as clean as possible on the field Post-op clean per manufacturer’s recommendations with proper enzymatic cleaning agent Rinse thoroughly with water Dry thoroughly including ports and channels
Use & Care of Endoscopes n n n High-Level Disinfection Intact mucous membranes Esophagoscope, colonoscope, bronchoscope, laryngoscope, cystoscope n n Sterilization Sterile/Intact tissue Vasculature Laparoscope, thoracoscope, arthroscope, angioscope
Use & Care of Endoscopes n n High Level Disinfection Gluteraldehyde FDA: soak 45 minutes Other: soak 20 minutes Rinse with sterile water (copious) *follow institution’s policy n n n Sterilization Ethylene Oxide Peracetic Acid (Steris) 30 minutes Should use soon after processed due to poor shelf life
Gastrointestinal Endoscopic Procedures n n n n Anoscopy- examination of the anal mucosa Choledochoscopy- examination of the common bile duct Colonoscopy- examination of the entire colon Esophagogastroduodenoscopy- (EGD)examination of the esophagus, stomach and duodenum Esophagoscopy- examination of the esophagus Gastroscopy- examination of the stomach Proctoscopy- examination of the rectum Sigmoidoscopy- examination of the sigmoid and rectum
Summary n n n Anatomy & Physiology, Pathology and Operative Considerations for: GI System Breast IVAD Care & Use of Endoscopes