Introduction to Antibacterial Therapy Clinically Relevant Microbiology and

Introduction to Antibacterial Therapy Clinically Relevant Microbiology and Pharmacology Edward L. Goodman, MD July 19, 2004
 leads to microbial resistance l Resistance results")
Rationale l Antibiotic use (appropriate or not) leads to microbial resistance l Resistance results in increased morbidity, mortality, and cost of healthcare l Appropriate antimicrobial stewardship will prevent or slow the emergence of resistance among organisms (Clinical Infectious Diseases 1997; 25: 584 -99. ) l Antibiotics are used as “drugs of fear” (Kunin CM Annals 1973; 79: 555)

Antibiotic Misuse l Surveys reveal that: – 25 - 33% of hospitalized patients receive antibiotics (Arch Intern Med 1997; 157: 1689 -1694) – 22 - 65% of antibiotic use in hospitalized patients is inappropriate (Infection Control 1985; 6: 226 -230)

Consequences of Misuse of Antibiotics l Contagious RESISTANCE – No equivalent downside to overuse of endoscopy, calcium channel blockers, etc. l Morbidity l Mortality l Cost - drug toxicity

Outline l Basic Clinical Bacteriology l Categories of Antibiotics l Pharmacology of Antibiotics

Goodman’s Scheme for the Major Classes of Bacterial Pathogens l Gram Positive Cocci l Gram Negative Rods l Fastidious GNR l Anaerobes

Gram Positive Cocci Gram stain: clusters l Catalase pos = Staph l Coag pos = S aureus l Coag neg = variety of species l Chains and pairs l Catalase neg = streptococci l Classify by hemolysis l Type by specific CHO l
 = penicillin resistant l At PHD ~50%")
Staphylococcus aureus >95% produce penicillinase (beta lactamase) = penicillin resistant l At PHD ~50% of SA are hetero (methicillin) resistant = MRSA l Glycopeptide (vancomycin) intermediate (GISA) l – MIC 8 -16 – Eight nationwide (one at PHD) l First VRSA reported July 5, 2002 MMWR – Third isolate reported May 2004 – MICs 32 - >128 – No evidence of spread in families or hospital
 [1970")
Evolution of Drug Resistance in S. aureus Penicillin Methicillin-resistant Penicillin-resistant S. aureus (MRSA) [1970 s] [1950 s] S. aureus [1997] Vancomycin [1990 s] Vancomycin- resistant S. aureus [ 2002 ] Vancomycin intermediateresistant S. aureus (VISA) Vancomycin-resistant enterococci (VRE)
")
MSSA vs. MRSA Surgical Site Infections (1994 - 2000)

Coagulase Negative Staph l Many species – S. epidermidis most common l Mostly methicillin resistant (65%) l Often contaminants or colonizers – use specific criteria to distinguish – Major cause of overuse of vancomycin
 Viridans streptococci (1%) Other (11%) SCOPE Project Coagulasenegative")
Nosocomial Bloodstream Isolates All gramnegative (21%) Viridans streptococci (1%) Other (11%) SCOPE Project Coagulasenegative staphylococci (32%) Candida (8%) Enterococci (11%) Staphylococci aureus (16%) Clin Infect Dis 1999; 29: 239 -244

Streptococci l Beta hemolysis: Group A, B, C etc. l Invasive – mimic staph in virulence l S. pyogenes (Group A) – Pharyngitis, – Soft tissue – Non suppurative sequellae: ARF, AGN
 – Peripartum/Neonatal – Diabetic foot")
Beta strept - continued l S. agalactiae (Group B) – Peripartum/Neonatal – Diabetic foot – Bacteremia/endocarditis/metastatic foci l Group D (non enterococcal) = S. bovis – Associated with carcinoma of colon

Viridans Streptococci l Many species l Streptococcus intermedius group – Liver abscess – Endocarditis – GI or pharyngeal flora l Most other are mouth flora – cause IE

Enterococci l l l l Formerly considered Group D Streptococci now a separate genus Bacteremia/Endocarditis Bacteriuria Part of mixed abdominal/pelvic infections Intrinsically resistant to cephalosporins No bactericidal single agent Role in intra-abdominal infection debated

Gram Negative Rods l l l Fermentors Oxidase negative Facultative anaerobes Enteric flora Numerous genera Non-fermentors l Oxidase positive l Pure aerobes l Pseudomonas and Acinetobacter l – Escherischia – Nosocomial – Enterobacter – Opportunistic – Serratia, etc – Inherently resistant

Fastidious Gram Negative Rods Neisseria, Hemophilus, Moraxella, HACEK l Require CO 2 for growth l Neisseria must be plated at bedside l – Chocolate agar with CO 2 – Ligase chain reaction (like PCR) has reduced number of cultures for N. gonorrhea l l Can’t do MIC without culture Increasing resistance to FQ

Anaerobes l Gram negative – Bacteroides – Fusobacteria rods l Gram positive rods – Clostridia – Proprionobacteria l Gram positive cocci – Peptostreptococci and peptococci

Anaerobic Gram Negative Rods l Produce beta lactamase l Endogenous flora l Part of mixed infections l Confer foul odor l Heterogeneous morphology l Fastidious

Antibiotic Classification according to Goodman l Narrow Spectrum – Active against only one of the four classes l Broad Spectrum – Active against more than one of the classes l Boutique – Active against a select number within a class

Narrow Spectrum l Active mostly against only one of the classes of bacteria – gram positive: glycopeptides, linezolid, daptomycin – aerobic gram negative: aminoglycosides, aztreonam – anaerobes: metronidazole

Narrow Spectrum GPC GNR Fastid Anaer ++++ ----- Linezolid ++++ ----- Daptomy ++++ cin AG ----- only clostridia Only gram pos ----- ++++ ++ ----- Aztreon ----- +++ + ----- Metro ----- ++++ Vanc

Broad Spectrum l Active against more than one class l GPC and anaerobes: clindamycin l GPC and GNR: cephalosporins, penicillins, T/S, newer FQ l GPC, GNR and anaerobes: ureidopenicillins ± BLI, carbapenems l GPC and fastidious: macrolides

Penicillins Strep OSSA GNR Fastid Anaer Pen +++ -- +/-- Amp/ amox Ticar +++ -- + +/-- ++ +/-- + Ureid +++ -- +++ ++ U+BLI +++ ++++ Carba ++++ +++

Cephalosporins FASTID ANAER Ceph 1 GPC non GNR -MRSA ++++ + -- -- Ceph 2 ++ ++ + -- Cephamycin Ceph 3 ++ +++ +++ -- Ceph 4 ++++ +++ --

Pharmacodynamics l MIC=lowest concentration to inhibit growth l MBC=the lowest concentration to kill l Peak=highest serum level after a dose l AUC=area under the concentration time curve l PAE=persistent suppression of growth following exposure to antimicrobial

Parameters of antibacterial efficacy l Time above MIC - beta lactams, macrolides, clindamycin, glycopeptides l 24 hour AUC/MIC - aminoglycosides, fluoroquinolones, azalides, tetracyclines, glycopeptides, quinupristin/dalfopristin l Peak/MIC - aminoglycosides, fluoroquinolones

Time over MIC l Should exceed MIC for at least 50% of dose interval l Higher doses may allow adequate time over MIC l For most beta lactams, optimal time over MIC can be achieved by continuous infusion (except unstable drugs such as imipenem, ampicillin)

Higher Serum/tissue levels are associated with faster killing l Aminoglycosides – Peak/MIC ratio of >10 -12 optimal – Achieved by “Once Daily Dosing” – PAE helps l Fluoroquinolones – 10 -12 ratio achieved for enteric GNR l PAE helps – not achieved for Pseudomonas – Not always for Streptococcus pneumoniae

AUC/MIC = AUIC l For Streptococcus pneumoniae, FQ should have AUIC >= 30 l For gram negative rods where Peak/MIC ratio of 10 -12 not possible, then AUIC should >= 125.

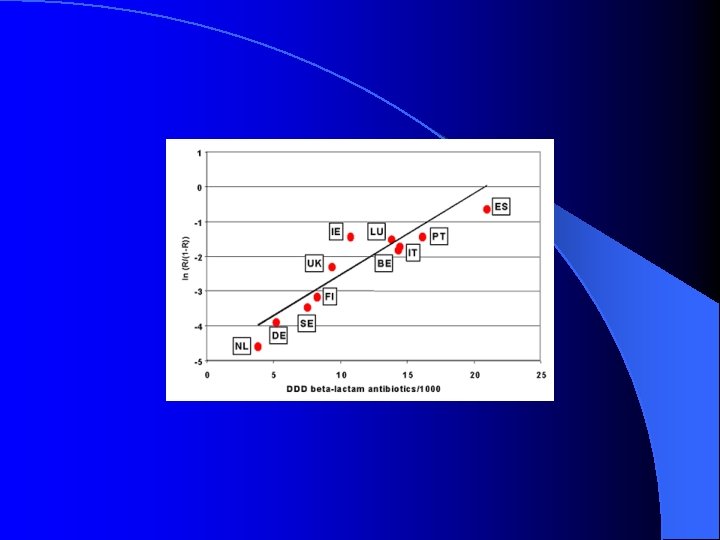
Antibiotic Use and Resistance l -Strong epidemiological evidence that antibiotic use in humans and animals associated with increasing resistance l -Subtherapeutic dosing encourages resistant mutants to emerge; conversely, rapid bactericidal activity discourages l -Hospital antibiotic control programs have been demonstrated to reduce resistance

Total Antibiotic Doses / Day

Changes in Bug/Drug Susceptibility Patterns

Other Activities of CAMP l Decrease inappropriate – Staff education – Restricted reporting l Decrease cultures fluoroquinolone use inappropriate sputum and urine – Staff education – Laboratory disclaimer l Decrease inappropriate vancomycin levels – Education about unnecessary peak levels

Further Activities of CAMP l Monitor surgical site infections and intervene as necessary – Improved timing and administration of pre-op antibiotics – clipping not shaving – nasal decolonization – changing pathogens (MRSA, gram- rods) l Automated protocol-driven antibiotic prescribing – Computerized physician order entry

Antibiotic Armageddon “There is only a thin red line of ID practitioners who have dedicated themselves to rational therapy and control of hospital infections” Kunin CID 1997; 25: 240

Historic overview on treatment of infections l 2000 BC: Eat this root l 1000 AD: Say this prayer l 1800’s: Take this potion l 1940’s: Take penicillin, it is a miracle drug l 1980’s: Take this new antibiotic, it is better l ? 2004 AD: Eat this root
- Slides: 39