Introduction Osmolality 2 Na Glucose18 BUN2 8 Disorder

Introduction § Osmolality = 2 Na + Glucose/18 + BUN/2. 8 § Disorder of serum Na § Disorder of water homeostasis § Change in relative ratio of Na to body water § Na homeostasis mechanism : Water intake & AVP Harrison’s 18 th edition

Hypernatremia

Introduction § Serum Na concentration > 145 mmol/L § Na is impermeable solute § Contributes to tonicity and induces water movement § Hypertonic hyperosmolality causes cellular dehydration § Net water loss § Majority of cases (Impaired of thirst or access to water gain) § Mental change, intubated, elderly, infants § Hypertonic sodium gain § Clinical intervention(Bivon), Accidental sodium loading

NEJM: 342, 1493 -1499, 2000

NEJM: 342, 1493 -1499, 2000

Clinical Manifestation § CNS dysfunction § Few symptoms until exceeds 160 mmol/L § Consciousness is correlated with the severity of hypernatremia § Lethargy, confusion, coma § Hypovolemia § Orthostatic hypotension, tachycardia § Brain shrinkage § Vascular rupture, Cerebral bleeding, SAH § Neurologic damage, death

Harrison’s 18 th edition

Treatment NEJM: 342, 1493 -1499, 2000

Treatment Harrison’s 18 th edition

Example § 58 -year old woman with postoperative ileus is undergoing nasogastric suction. Obtunded and diminished skin turgor. - Na: 158, K: 4. 0, Wt. : 63 kg § 5 DW fluid § Na change = (0 – 158) / (63 x 0. 5 +1) = - 4. 86 § 1000 ml : -4. 86 = x : 10 § X = 2057 ml → 2057 ml/24 hr § 85. 7 ml/hr for 24 hrs

NEJM: 342, 1493 -1499, 2000

Hyponatremia

Harrison’s 17 th edition

Harrison’s 18 th edition
 § GI loss (vomiting, diarrhea,")
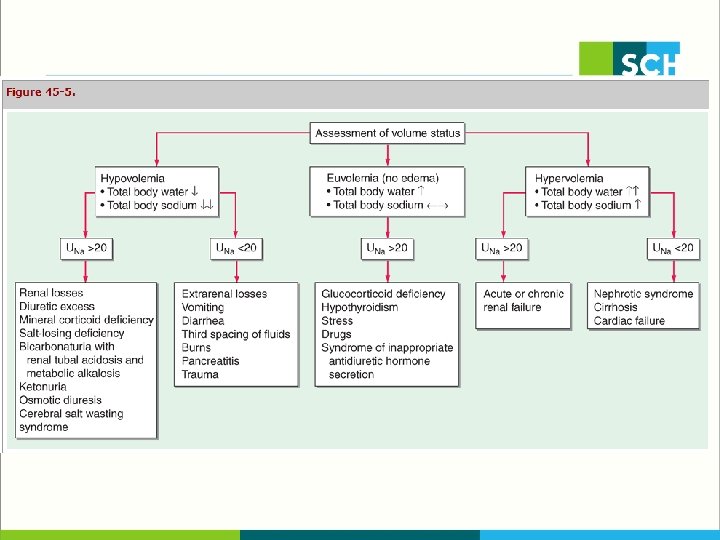
Hypovolemic § Extrarenal loss (Urine Na < 20 ) § GI loss (vomiting, diarrhea, tube drainage) § Insensible loss (sweating, burn) § Renal loss (Urine Na > 20 ) § Primary adrenal insufficiency, Hypoaldosteronism § Salt-losing nephropathies § Thiazide : not inhibit the renal concentrating mechanism (cf. Lasix : blunt the countercurrent reducing urine concentration) § Osmotic diuresis : glycosuria, ketonuria, bicarbonaturia

Hypervolemic § Heart failure, Cirrhosis, Nephrotic syndrome § Pathogenesis § Increase total body Na. Cl with greater increase total body water § Decreased effective volume, Increased AVP → Volume overload § Urine sodium is very low even after N/S hydration § Increased urine Na § Acute or chronic renal failure § The degree of hyponatremia § Important prognostic factors
 § Secondary adrenal insufficiency")
Euvolemic § Mod to severe hypothyroidism (CO & GFR ↓) § Secondary adrenal insufficiency (Cortisol inhibits ADH) § SIADH § m/c cause of euvolemic hyponatremia § Unregulated AVP secretion, Not suppressed at lower osmolality § SIADH causes § Pulmonary disease (pneumonia, TBc, pleural effusion) § CNS disease (tumor, SAH, meningitis) § Malignancy (SCLC : 75%) § Drugs (m/c SSRI)

Harrison’s 18 th edition
- Slides: 20