Introduction Operative vaginal delivery OVD refers to a

 refers to a vaginal birth with the use of")














- Slides: 19
Introduction
� Operative vaginal delivery (OVD) refers to a vaginal birth with the use of any type of forceps or vacuum extractor (ventouse). The terms instrumental delivery, assisted vaginal delivery and OVD are used interchangeably. The goal of OVD is to expedite delivery with a minimum of maternal or neonatal morbidity. As with other forms of intrapartum intervention, OVD should only be performed when the safety criteria have been met and when the benefits outweigh the risks.
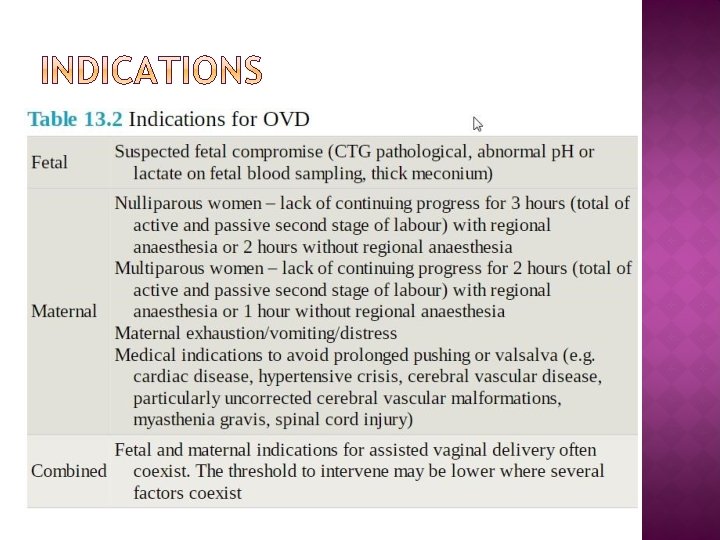
The indications for OVD can be divided into fetal or maternal, although in many cases these factors coexist. The most common fetal factor is suspected fetal compromise, usually based on a pathological cardiotocograph (CTG). The most common maternal factor is a prolonged active second stage of labour. The underlying aetiology for a prolonged second stage should be evaluated in terms of the 3 Ps.
Depending on the overall clinical findings it may be appropriate to use an oxytocin infusion, change the maternal position and offer further encouragement or proceed directly to instrumental delivery. In some cases the findings will be a contraindication to OVD and favour delivery by caesarean section. The indications are summarized in the following table.
The guidelines of the RCOG recommend that obstetricians should be competent and confident in the use of both forceps and the ventouse and that practitioners should choose the most appropriate instrument for the individual circumstances. The choice of instrument should be based on a combination of indication, experience and training. The aim should be to complete the delivery successfully with the lowest possible morbidity and, where appropriate, the preferences of the mother should be taken into account.
Ventouse and forceps have been compared in a number of RCTs analysed within a Cochrane systematic review. The incidence of maternal pelvic floor trauma in deliveries performed with the ventouse is less than with forceps; anal sphincter injury in particular is twice as common with forceps delivery (8% versus 3– 4%). Ventouse delivery is preferred as a first-line instrument by many obstetricians in terms of reduced maternal trauma, but this needs to be balanced with a failure rate of 10– 20% compared to a failure rate with forceps of 5% or less for similar deliveries.
The ventouse compared to forceps is significantly more likely to be associated with: 1. Failure to achieve a vaginal delivery. 2. Cephalohaematoma (subperiosteal bleed). 3. Retinal haemorrhage. 4. Maternal worries about the baby.
The ventouse compared to forceps is significantly Less likely to be associated with: 1. Use of maternal regional/general anaesthesia. 2. Significant maternal perineal and vaginal trauma. 3. Severe perineal pain at 24 hours.
The ventouse compared to forceps is similar in terms of: 1. Delivery by caesarean section (where failed vacuum is completed by forceps). 2. Low 5 minute Apgar scores.
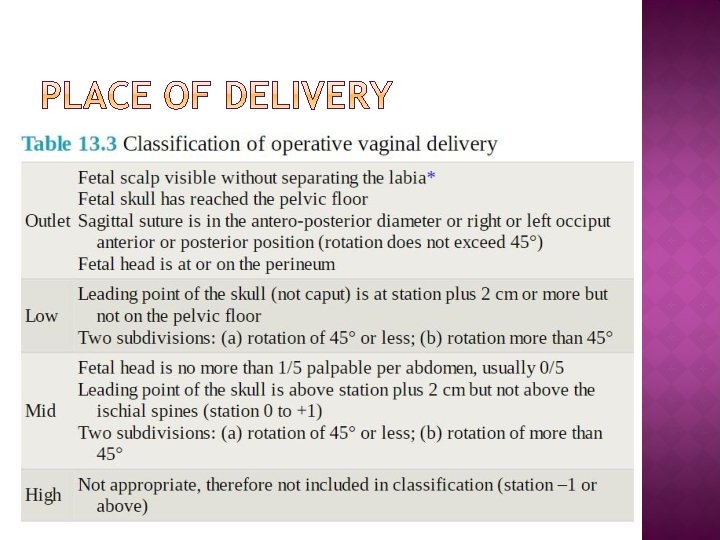
OVDs in the midpelvis are more difficult either because there is a malposition and rotation is required or there is a degree of relative CPD (Table 13. 3). These deliveries require a higher degree of skill and there is inherent uncertainty whether OVD can be achieved safely. The alternative is to deliver by caesarean section, which can also be a very challenging procedure with the head deep in the pelvis.
The anatomy of the birth canal and its relationship to the fetal head must be understood to become skilled in the safe use of forceps or ventouse
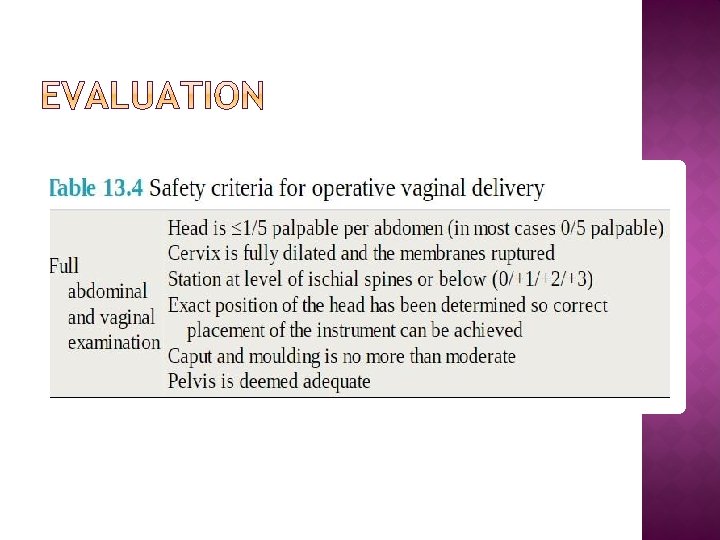
A full abdominal and vaginal examination should take place to confirm the fetal lie, presentation, engagement, station, position, attitude and degree of caput or moulding. This will confirm whether or not the basic safety criteria for OVD have been met. A careful pelvic examination is also essential.
Analgesic requirements are greater forceps than for ventouse delivery. Where rotational forceps or midpelvic direct traction forceps are needed, regional analgesia is preferred. For a rigid cup ventouse delivery, a pudendal block with perineal infiltration may be all that is needed and if a soft cup is used, analgesic requirements may be limited to perineal infiltration with local anaesthetic.
OVDs are traditionally performed with the patient in the lithotomy position. The angle of traction needed requires that the bottom part of the bed be removed. In patients with limited abduction (such as those with symphysis pubis dysfunction), it may be necessary to limit abduction of the thighs to a minimum. It is the operator’s duty to ensure that the bladder is emptied.
With any OVD there is the potential for failure with the chosen instrument and the operator must have a back-up plan for such an event. It may be possible to complete a failed vacuum delivery with low-pelvic forceps, but failed or abandoned forceps delivery will almost always result in caesarean section.
Done by : Amro Hamad Reference : Obstetrics by ten teachers 20 th edition