Introduction 1 The only pathogenic amoeba among all


Introduction 1. The only pathogenic amoeba among all of the intestinal amoebae 2. Infecting perhaps 10% of the world's population. 3. Lead to invasive amoebiasis.
 – 5% in")
Entamoeba histolytica Entamoeba dispar l Major pathogen – world-wide distribution (10%) – 5% in some developed countries – 100 deaths in Chicago 1930 l Trophozoite & Cyst – oral-faecal transmission

Morphology l Pay your attention to stages that have diagnostic value Parasites stained with hematoxylin is described here.
 (1) Size: 10 -40 micrometers in diameter, some are above 60")
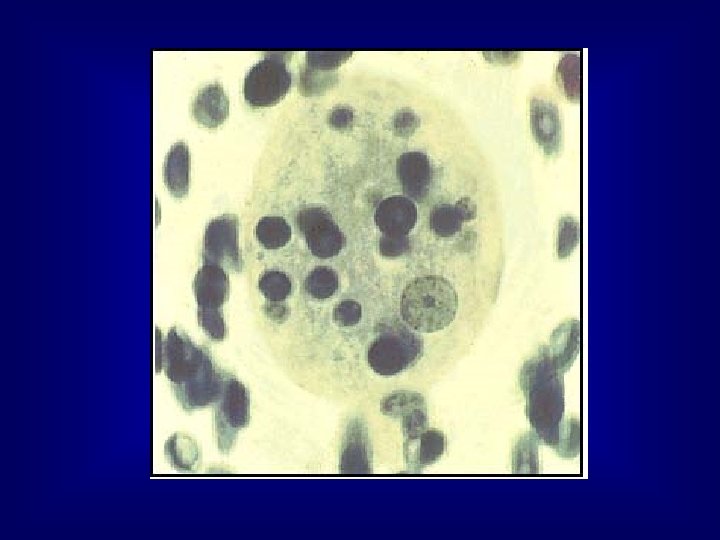
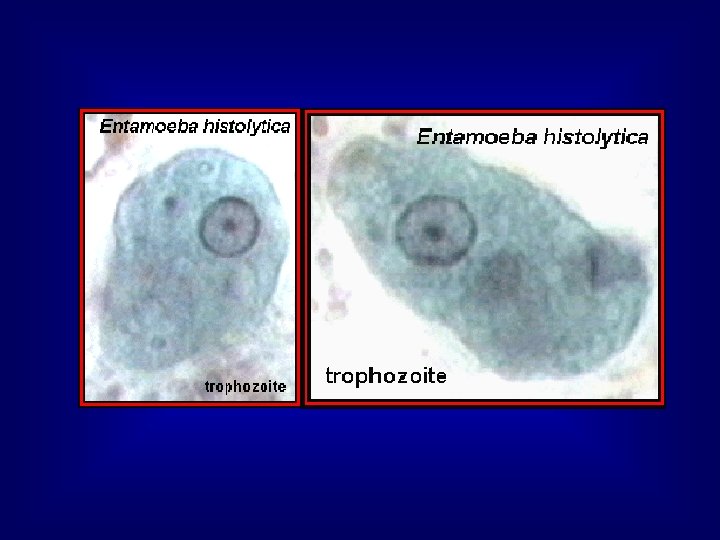
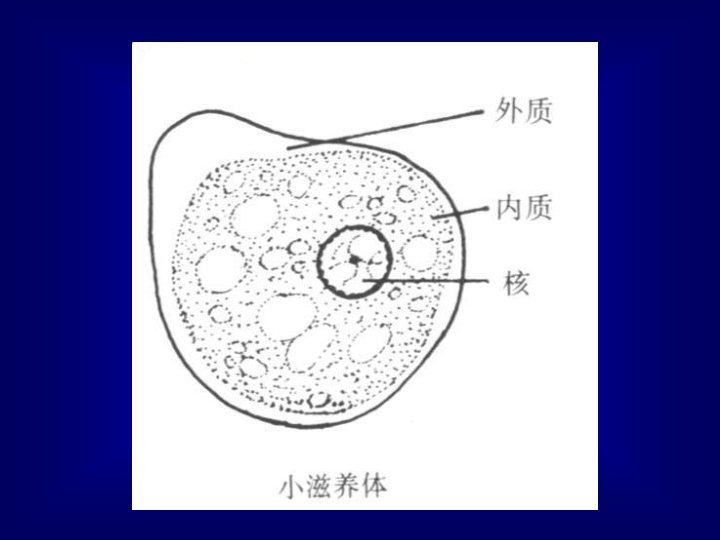
Trophozoite (active form) (1) Size: 10 -40 micrometers in diameter, some are above 60 micrometers. l (2) Pseudopodium(ectopalsmic protrusion): A. broad or finger-like in form B. thrust out quickly C. firstly, formed with ectoplasm, secondly, endoplasm flows slowly into it. D. motility is progressive and directional. l
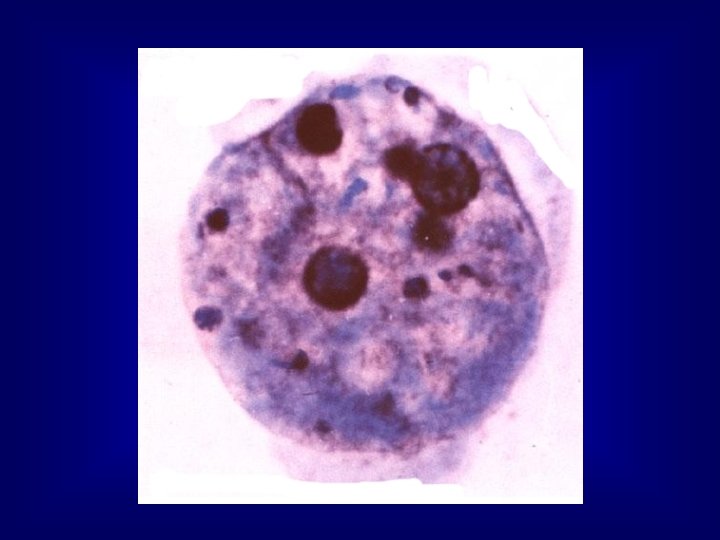
 (3) Endoplasm: red blood cells may be found in it. l")
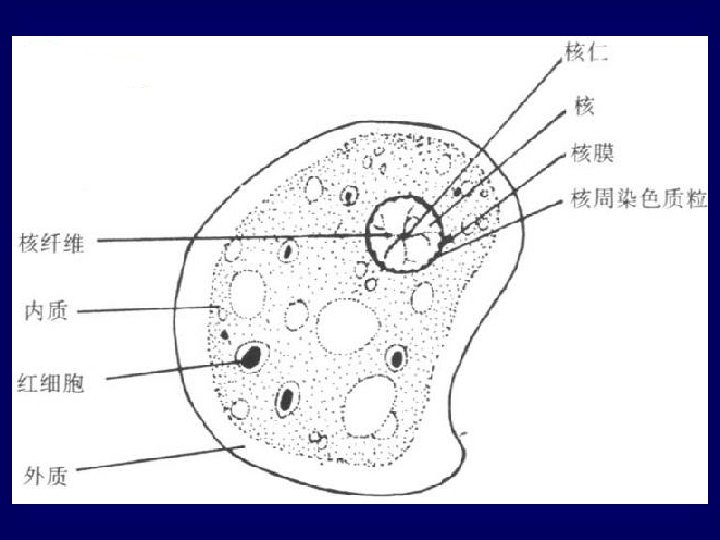
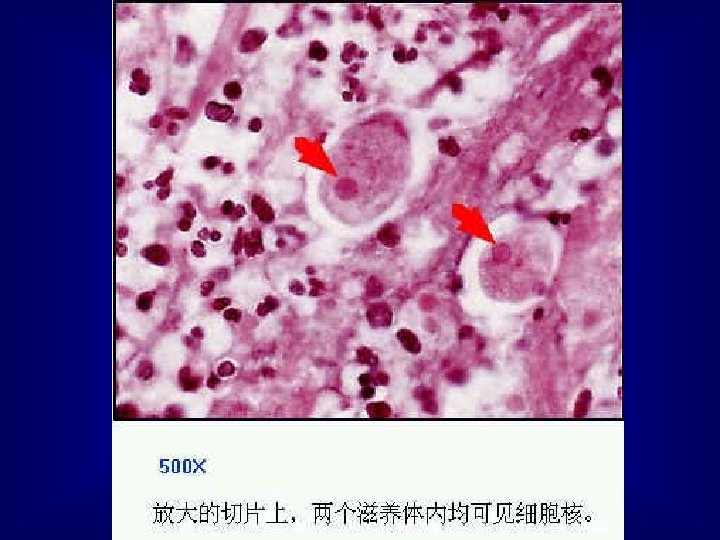
Trophozoite (active form) (3) Endoplasm: red blood cells may be found in it. l (4) Nucleus (vesicular type) It is not visible in an unstained specimen; but its clear structure can be seen when stained with hematoxylin. A: membrane: distinct line B: chromatin granules: fine and uniformly arranged in the inner surface of the nuclear membrane. C: karyosome: small and centrally located. l

Phase contrast photomicrograph of cultured Entamoeba histolytica trophozoites.

Charcot Leyden Crystal l These diamond shaped crystals are often seen in amoebic dysentery faeces and may also be present in other parasitic infections. They are absent in bacillary dysentery. Interference contrast. × 400. Enlarged by 9. 6

Movement of E. histolytica 进行性和定向阿米巴运动 progressive and directional
 (1) 10 -20 mocrometers in size l (2) spherical in shape l")
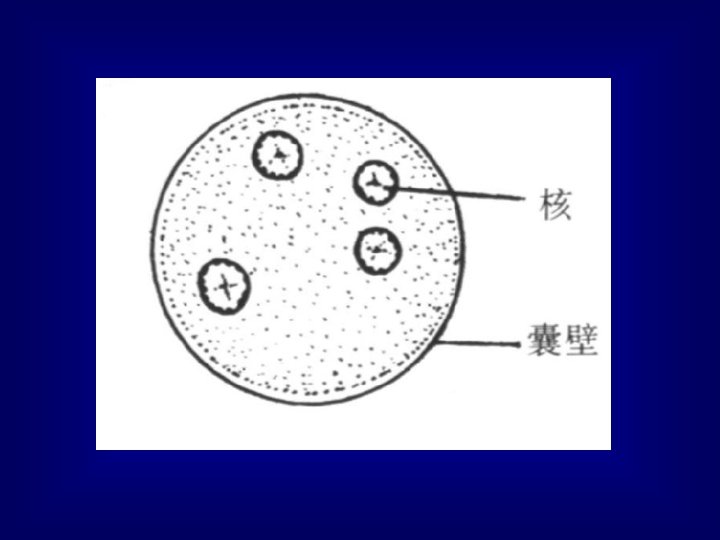
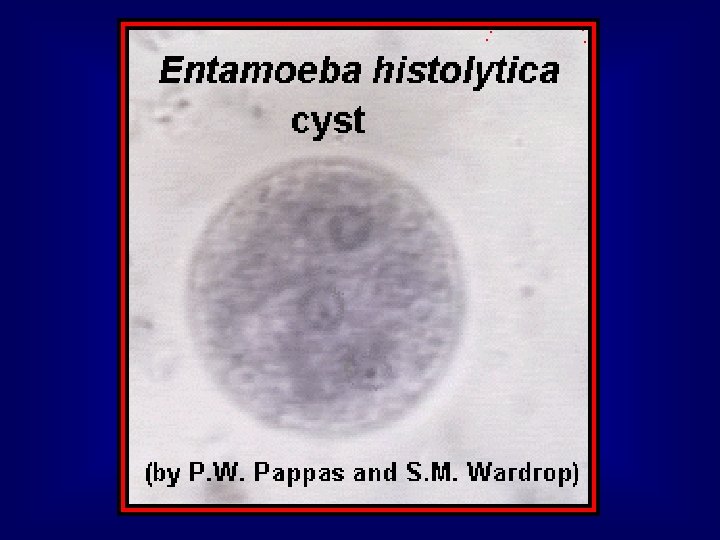
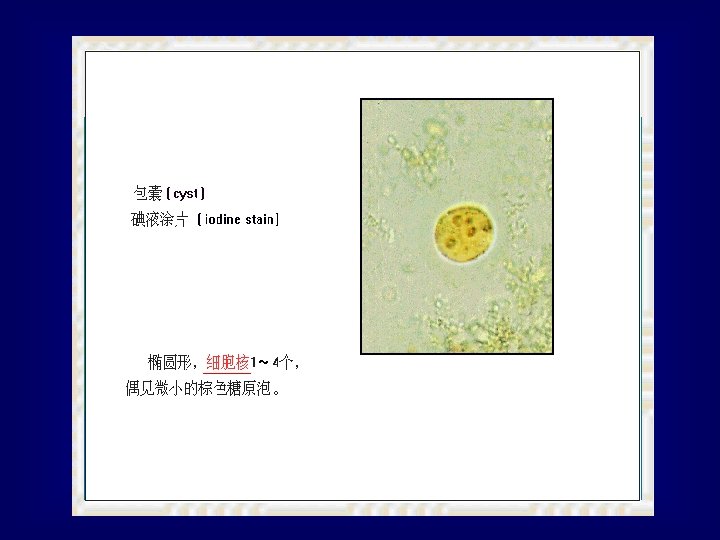
Cyst (non-motile) (1) 10 -20 mocrometers in size l (2) spherical in shape l (3) 1 -2 nuclei (immature cyst); 4 nuclei (mature cyst-infective stage). l (4) inclusions: (become smaller and smaller as the cyst ages) glycogen vacuole appears as a clear space; food reservoir chromatoid body dark blue rods or dots; its function is not known
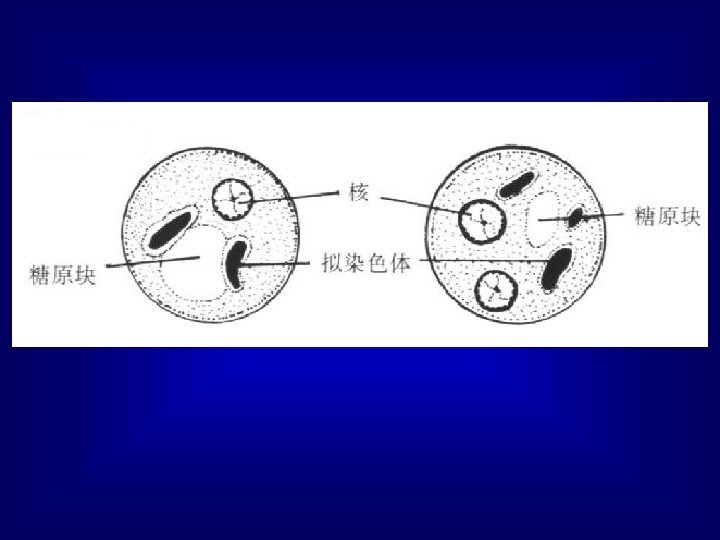

l The single nucleus with its central endosome and regularly distributed chromatin is visible. The dark "rods" in the cytoplasm are the chromatoid bars; approximate size = 18 µm.

l This is a mature cyst and contains four nuclei. However, only two nuclei are visible in this plane of focus, and a chromatoid bar is still present; approximate size = 17 µm.

Entamoeba coli l Gut commensal l Trophozoite & cyst l Slow “lazy” movement l Oral-faecal transmission

E. histolytica v E. coli l Trophozoite – 10 -40 um – 15 -30 um – delicate nuclear – coarse nuclear structure l structure Cyst – 9. 5 -15. 5 um – 10 -30 um – 4 nuclei – 8 nuclei – Broad, blunt chromatid – thin, sharp chromatid bodies

Entamoeba coli

Entamoeba coli

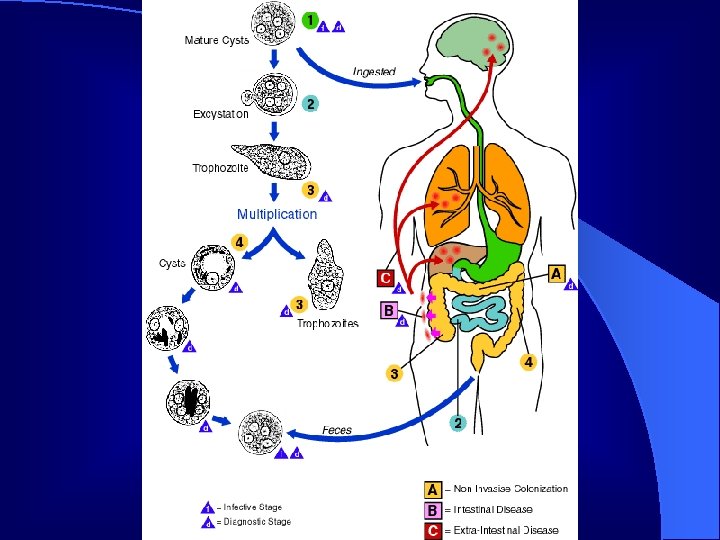
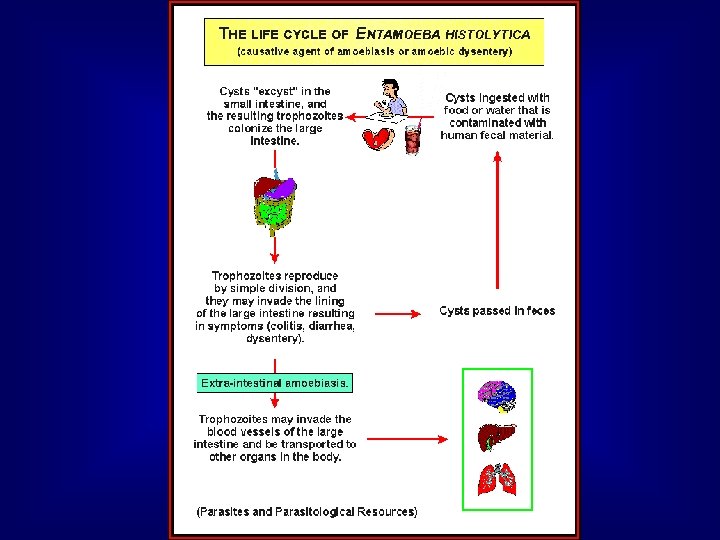
Life Cycle l 1 infective stage: mature cyst l 2 access: mouth l 3 ecological niches: large intestine; liver, lung and other organs. l 4 pathogenic stage: trophozoite l 5 diagnostic stage: cyst; trophozoites

Pathogenic factors l 1. Toxicity of parasites pathogenic- nonpathogenic complex. l Entamoeba histolytica Entamoeba dispar l 2. Symbiotic bacteria l 3. Defence barrier immunity

l. This cytolytic event is a result of incorporation in the host cell membrane of an ameba-produced, pore-forming protein, Amoebapore. l. This protein forms ion channels in lipid cell membranes and results in cell death within minutes of cell contact with the ameba. Amoebapore has been isolated, synthesized and well characterized. Non-pathogenic strains of E. histolytica can also produce amoebapore but are much less efficient at its production and the molecule is not exactly similar to that produced by virulent strains.

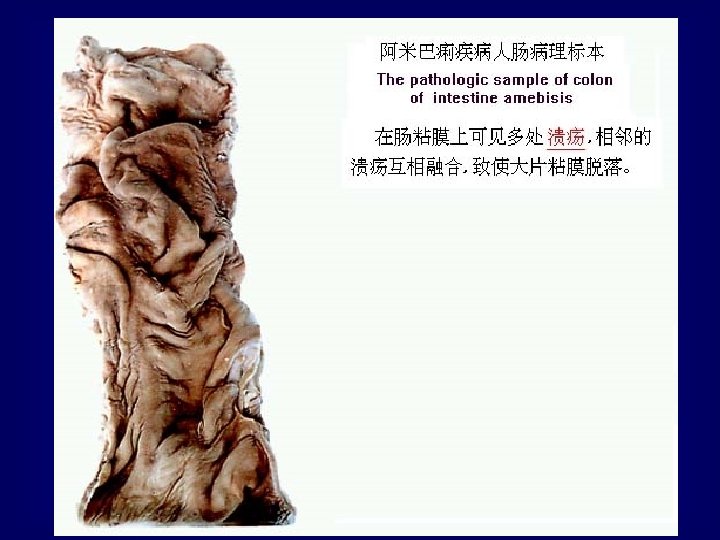
Pathology and Clinical Manifestation l Pinpoint lesion on mucous membrane l Flask-shaped crateriform ulcers
 >90% cases (E. dispar? ) l Sympomatic cases")
Clinical classification l Asymptomatic infection (carrier) >90% cases (E. dispar? ) l Sympomatic cases <10% – 8 -10% dysentery, colitis, etc – 2% invasive amoebiasis – 0. 1% deaths
.")
A. Intestinal amoebiasis a. dysentery: dysenteric stools (pus and blood a. dysentery: without feces). fever, dehydration, and electrolyte abnormalities. Tenesmus and abdominal tenderness. l b. non-dysenteric colitis l c. appendicitis l d. amoeboma: may become the leading point of an intussusception or may cause intestinal obstruction. l

Histopathology of a typical flask-shaped ulcer of intestinal amebiasis
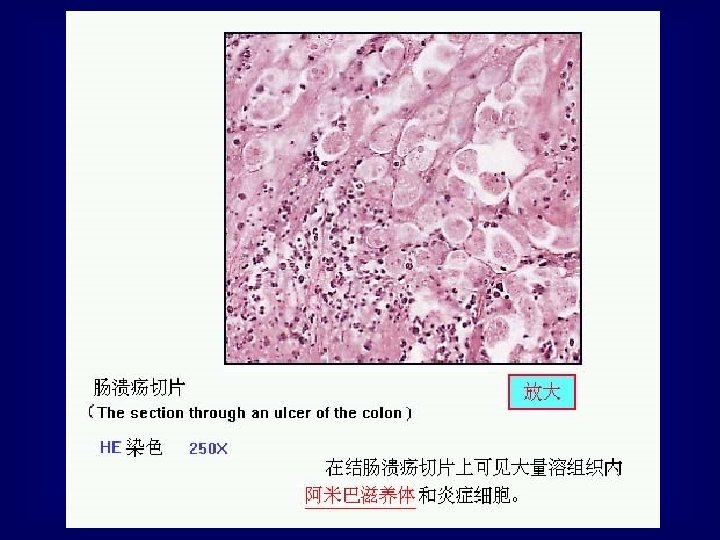

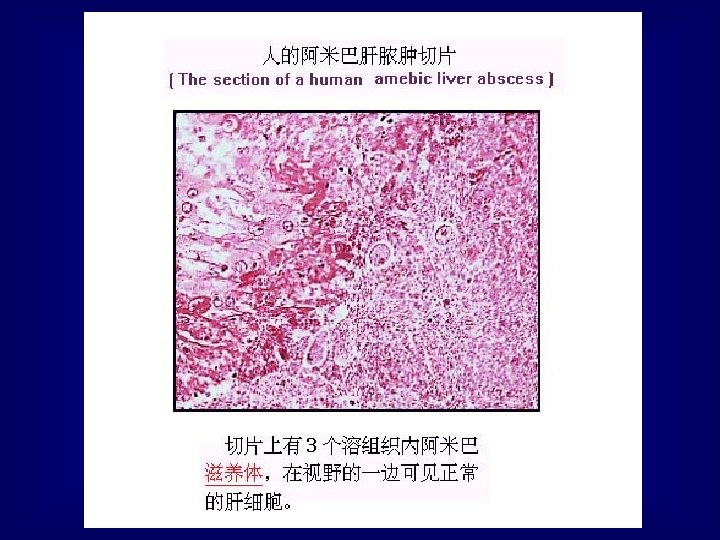
A Micro Abscess in the submucosa. l Containing a large number of E. histolytica trophozoites mostly at the periphery. H and E. × 400. Enlarged by 5. 4.
 acute non-suppurative l (2) liver abscess:")
B. Extra-intestinal amoebiasis l a. Hepatic l (1) acute non-suppurative l (2) liver abscess: right upper quadrant pain, referred to the right shoulder. tender. l b. Pulmonary

B. Extra-intestinal amoebiasis l c. Brain l d. Skin, perianal infection l e. Other extra-intestinal amoebiasis

Amoebic Liver Abscess

Gross pathology of liver containing amebic abscess

Gross pathology of amebic abscess of liver. Tube of "chocolate" pus from abscess.

An Amoebic Liver Abscess Being Aspirated. l Note the reddish brown color of the pus (‘anchovy-sauce’). This color is due to the breakdown of liver cells. Enlarged by 5. 4

X-ray of a Large Amoebic Liver Abscess. l A fluid level has formed after aspiration due to entry of air

Diagnosis 1. Stool examination specimen trophozoite cyst feces method direct smear with normal saline direct smear with iodine stain diseases amoebic dysentery chronic intestinal amoebiasis or carriers remarks 1. container must clean 2. examined soon after they 4. keep specimen warm. have been passed. 3. select bloody and 5. drug using histry. mucous portion.

Diagnosis l 2. Serologic studies: indirect hemagglutination, skin tests, ELISA and latex agglutination. l 3. Tissue examination: sigmoidoscopic biopsy, aspiration l 4. DNA probe

Epidemiology l Distribution: all climates, arctic to tropical. Media: flies; black beetles etc.

Treatment and Prevention l Treatment: l Diodoquin-carriers l Metronidazole-dysentery, liver abscess

Prevention l Human feces should not be used as fertilizer l Food and drinks must be protected from flies l Personal hygiene: wash hands after defecation and before meals.
- Slides: 53