Intraventricular hemorrhage IVH Andrea MartelBucci NNP Outline What
 Andrea Martel-Bucci, NNP")
Intraventricular hemorrhage (IVH) Andrea Martel-Bucci, NNP

Outline • What is it? • Who is at risk and why? • What are the complications? • What are the outcomes/prognosis? • How can we prevent it?

What is it? Major neurological complication of PREMATURITY

What is it? • Bleed that typically initiates in the periventricular GERMINAL MATRIX • Highly vascularized portion of the FETAL brain which produces brain cells

What is it? • Why is the germinal matrix predisposed to bleeding? • +++ blood vessels • Capillary bed characteristically different • Venous drainage

WHO IS AT RISK? PRETERM INFANTS Presence of germinal matrix & immature brain So why do some preemies get it and others not? ?

Risk factors • PRENATAL • POSTNATAL • Maternal infection and chorioamnionitis • • Protective prenatal factors: • • Antenatal steroids (betamethasone) • • • Prematurity Birth outside of tertiary care center Need for resuscitation at birth RDS, intubation, mechanical ventilation Hypo/hypercarbia Mechanical ventilation Coagulation and platelet abnormalities BP fluctuations & fluid boluses Caretaking procedures Sepsis NEC Need for surgery

Incidence

Clinical presentation • Silent presentation – 25 to 50 percent of cases; detected by routine ultrasound screening • Saltatory or stuttering course is the most common presentation and evolves over hours to several days. It is characterized by nonspecific findings including an altered level of consciousness, hypotonia, decreased spontaneous and elicited movements, and subtle changes in eye position and movement. Respiratory function is sometimes disturbed. • Catastrophic deterioration is the least common presentation and evolves over minutes to hours. Signs include: Stupor or coma Irregular respirations, hypoventilation, or apnea Decerebrate posturing Generalized seizures, especially tonic seizures Flaccid weakness Cranial nerve abnormalities, including pupils fixed to light • Other features include a bulging anterior fontanelle, hypotension, bradycardia, a falling hematocrit, metabolic acidosis, and inappropriate antidiuretic hormone secretion • • •

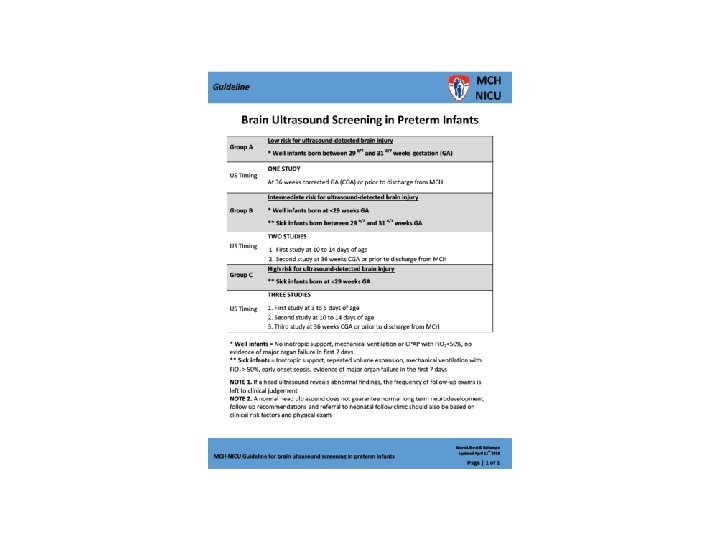
Who do we screen and when?

WHO DO WE SCREEN & WHEN?

DIAGNOSIS Brain ultrasound Brain MRI/CT

GRADING SYSTEMS PAPILE VOLPE

Images: what does normal look like?

What grade? Left GRADE I

What grade? Right GRADE II

What grade? Left GRADE III, Right GRADE II

What grade? BILATERAL GRADE IV

MAJOR COMPLICATIONS • Short term: • Hydrocephalus/post hemorrhagic ventricular dilatation • Anemia, acidosis • Long term: • PVL (periventricular leukomalacia) • Cerebral palsy, motor deficits

hydrocephalus • Excessive accumulation of fluid in the brain • Results in abnormal widening of ventricles

PVL • Periventricular leukomalacia • … characterized by the death of the white matter of the brain due to softening of the brain tissue. It can affect fetuses or newborns; premature babies are at the greatest risk of the disorder. PVL is caused by a lack of oxygen or blood flow to the periventricular area of the brain, which results in the death or loss of brain tissue.

Cerebral palsy Static encephalopathy leading to an evolving motor impairment * Spastic diplegia most common

PROGNOSIS & OUTCOMES • Grade I and grade II hemorrhage: Neurodevelopmental prognosis is excellent (ie, perhaps slightly worse than infants of similar gestational ages without PVHIVH). • Grade III hemorrhage without white matter disease: Mortality is less than 10%. Of these patients, 30 -40% have subsequent cognitive or motor disorders. • Grade IV IVH with either periventricular hemorrhagic infarction and/or periventricular leukomalacia (PVL): up to 90% incidence of neurological sequelae including cognitive and motor disturbances

Prevention Pharmacologic • Antenatal steroids • Antenatal magnesium sulfate ? • Indomethacin prophylaxis Non-pharmacologic • Birth of premature babies in tertiary care centers • Resuscitation at birth by experienced personnel / golden hour • Restoration of normal oxygenation and ventilation • Avoid fluid boluses/ inotropes • Gentle and synchronized ventilation • MINIMAL HANDLING

Questions?
- Slides: 26