INTRAVENTRICULAR CONDUCTION DISTURBANCES AHAACCFHRS RECOMMENDATIONS FOR THE STANDARDIZATION

INTRAVENTRICULAR CONDUCTION DISTURBANCES AHA/ACCF/HRS RECOMMENDATIONS FOR THE STANDARDIZATION AND INTERPRETATION OF IVCD JACC 2009 VOL 53

Normal QRS Duration ↑with ↑ heart size Wider - precordial Age- and gender-dependent Children <4 yrs -QRS ≥ 90 ms prolonged 4 -16 yrs –QRS ≥ 100 ms prolonged Adult males – N-QRS up to 110 ms • > limb leads J. Am. Coll. Cardiol. 2009; 53; 976 -981;

Mean Frontal Plane Axis • J. Am. Coll. Cardiol. 2009; 53; 976 -981;

Shifts to the left with increasing age
, >100 ms (4 -16 yrs),")
Complete RBBB q QRS ≥ 120 ms (>16 yrs), >100 ms (4 -16 yrs), >90 ms (<4 yrs) q rsr’, rs. R’, or Rsr’ - V 1 or V 2. R’/r’ - Usually wider than initial R/r q S duration > R or >40 ms (I&V 6) q Normal R peak time (V 5 & V 6) but >50 ms (V 1) First 3 should be present to make diagnosis o V 1 - pure dominant R wave ± notch → Criterion 4 should be satisfied • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
, 90 - 100 ms (8 -16")
Incomplete RBBB QRS duration 110 -120 ms (adults), 90 - 100 ms (8 -16 yrs), 86 - 90 ms (<8 yrs) Other criteria - Same as for complete RBBB. Children –incomplete RBBB when terminal rightward deflection is less than 40 ms and greater than or equal to 20 ms In the absence of heart disease –incomplete RBBB can occu rwhen V 1 is placed higher or to the right from normal posistion • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
, >100 ms (4 -16), >90 ms")
Complete LBBB 1. QRS ≥ 120 ms (Adults), >100 ms (4 -16), >90 ms ( <4) 2. Broad notched /slurred R wave - I, a. VL, V 5, V 6 3. Absent q waves - I, V 5, V 6 (±q Avl) 4. R peak time > 60 ms in V 5 & V 6 but Normal in V 1, V 2, & V 3 (when r is present) 5. ST & T - Usually opposite in direction to QRS 6. + T wave with upright QRS may be N (+ concordance) 7. ST depression and/or −T with −QRS (- concordance) -ABN • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
 ST↑≥ 0. 1")
Criteria for infarction in the presence of complete left bundle-branch block(GUSTO) ST↑≥ 0. 1 m. V in leads with +QRS (concordant ST) ST ↑≥ 0. 5 m. V in leads with −QRS (discordant ST) ST ↓≥ 0. 1 m. V in V 1 -V 3 (concordant ST) Concordant ST changes -↑specificity but ↓ sensitivity Discordant ST changes - ↓↓ specificity ↓↓ sensitivity LBBB + concordant ST > 30 -d mortality > LBBB + enzyme -- concordant ST changes • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
, 90 - 100 ms(8 -16), 80")
Incomplete LBBB 1. QRS 110 -120 ms (adults), 90 - 100 ms(8 -16), 80 - 90 ms (<8) 2. Presence of LVH pattern 3. R peak time >60 ms in leads V 4, V 5, and V 6 4. Absent q in I, V 5, V 6 • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
, >90 ms (8 -16), >80 ms")
Nonspecific/Unspecified Intraventricular Conduction Disturbance QRS >110 ms (adults), >90 ms (8 -16), >80 ms (<8) without criteria for RBBB or LBBB Also RBBB criteria in precordial leads and LBBB criteria in limb leads, and vice versa • J. Am. Coll. Cardiol. 2009; 53; 976 -981;

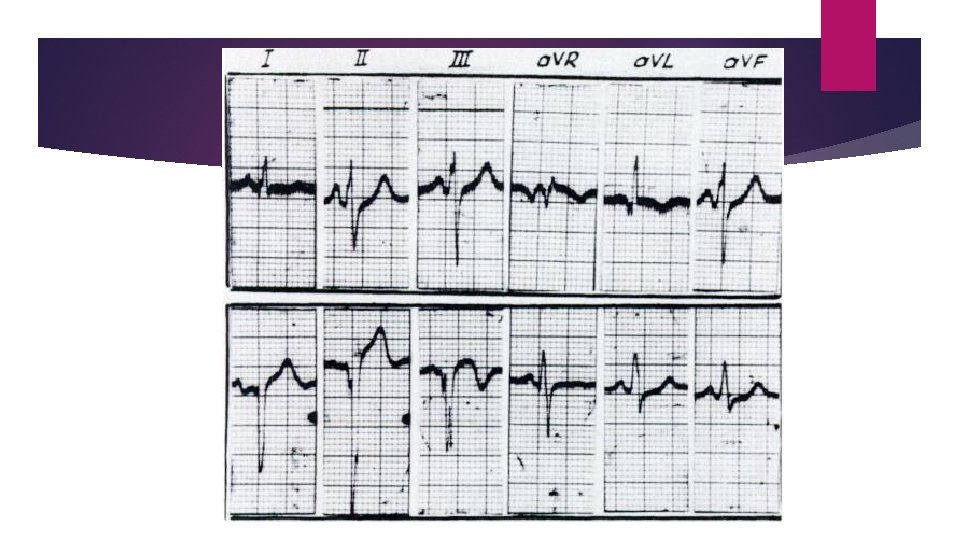
Left Anterior Fascicular Block 1. Frontal plane axis -45°to -90° 2. q. R pattern in a. VL 3. R-peak time in a. VL of ≥ 45 ms 4. QRS duration <120 ms These criteria do not apply to patients with CHD in whom LAD is present in infancy • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
 2. r. S")
Left Posterior Fascicular Block 1. Frontal plane axis +90°to 180° (adults) 2. r. S pattern in I and a. VL 3. q. R pattern in III and a. VF 4. QRS <120 ms • J. Am. Coll. Cardiol. 2009; 53; 976 -981;

Terms Not Recommended Mahaim-type preexcitation -because ∆ cannot be made with certainty with surface ECG Atypical LBBB, bilateral bundle-branch block, bifascicular block, and trifascicular block -because of great variation in anatomy and pathology producing such patterns Recommends that each conduction defect be described separately in terms of the structure or structures involved • J. Am. Coll. Cardiol. 2009; 53; 976 -981;

Peri-infarction block abnormal Q wave generated by a MI in Inf/lat leads, terminal portion of QRS- wide and directed opposite to Q wave (i. e. , a QR complex in the inferior or lateral leads) • J. Am. Coll. Cardiol. 2009; 53; 976 -981;
- Slides: 15