INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician





 •")
 • Isotonic (‘normal’) 0. 9% saline +/-")
 – osmolality 308 m. Osmol/L")
 Plasma 0. 9% Saline Hartmann’s Plasmalyte 148 5%")






 Wet (Liberal)")
 Wet (Liberal) d i lu rg’")




- Slides: 23
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician
LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal about ‘Normal’ Saline? 5. Goals of fluid therapy 6. Recognizing and managing hypovolaemia 7. Daily electrolyte and fluid requirements 8. Maintenance, Replacement and Redistribution 9. Summary: The 5 Rs and NICE CG 174
WHAT IS THE PROBLEM WITH FLUID THERAPY? ‘Cautious IV Fluids…. . Because the patient has angina? !’
THE ‘POPCORN’ MODEL OF FLUID THERAPY Daily fluid requirement = +
QUESTIONS TO ASK BEFORE PRESCRIBING FLUID 1. Does my patient need IV fluid? 2. For what purpose? 3. What type of fluid? 4. What amount (volume) of fluid? 5. What rate (how fast)? > POLL ENGAGE BRAIN!
} DAILY ELECTROLYTE REQUIREMENTS 1. Sodium • 1 -2 mmol/kg/d (70 -140 mmol/d) • Serum concentration 140 mmol/L 2. Potassium • 0. 5 -1 mmol/kg/d (35 -70 mmol/d) • Serum concentration 4 mmol/L 3. Chloride • 1 mmol/kg/d (70 mmol/d) • Serum concentration 100 mmol/L 1 mmol/kg/d of each
WHAT’S IN YOUR CUPBOARD? 1. Crystalloids (hopefully) • Isotonic (‘normal’) 0. 9% saline +/- 20 -40 mmol KCl • Hartmann’s solution • 5% and 10% glucose • 4% glucose/0. 18% saline (‘dex-saline’) +/- 20 -40 mmol KCl • Plasmalyte 148 (if you are lucky) 2. Colloids (possibly) • Albumins • Gelatins e. g. Gelofusine®, Volplex® • Starches > POLL
WHAT’S NORMAL ABOUT ‘NORMAL’ SALINE? • Tonicity (‘isotonic’…. almost) – osmolality 308 m. Osmol/L (plasma 275295 m. Osmol/L) …. . and not a lot else! • Sodium 154 mmol/L (140 mmol/L) • Chloride 154 mmol/L (100 mmol/L) • p. H 5. 5 (7. 4) • Potassium 0 mmol/L (4 mmol/L) > POLL
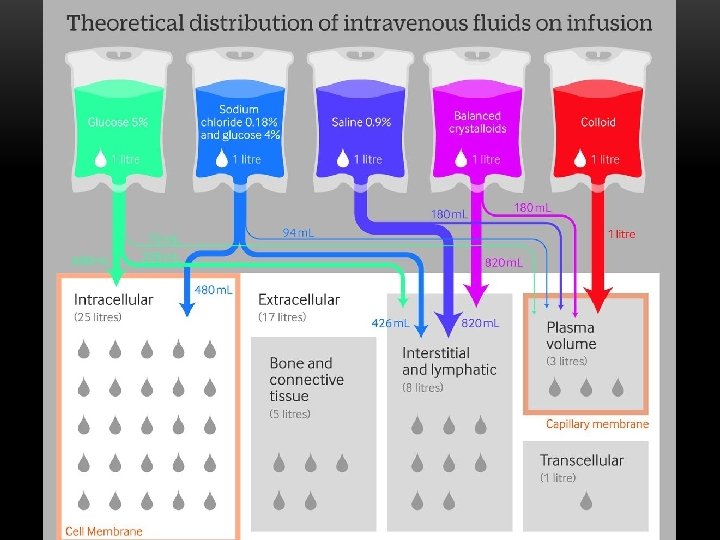
COMPOSITION OF DIFFERENT CRYSTALLOIDS Content (mmol/L) Plasma 0. 9% Saline Hartmann’s Plasmalyte 148 5% Glucose 0. 18% Saline-4% Glcuose Sodium 140 154 131 140 0 31 Potassium 4 0 5 5 0 0 Chloride 100 154 111 98 0 31 Lactate etc. <2 0 29 0 (gluconate 23, acetate 27) Calcium 2. 4 0 2 0 (Mg 1. 5) 0 0 Glucose 4. 5 0 0 0 278 (50 g) 222 (40 g) p. H 7. 4 5. 5 6. 0 4. 5 Osmolality 285 308 278 295 278 284 0
WHAT HAPPENS IF YOU GIVE ‘NORMAL’ SALINE? • p. H depends on difference between strong +ve ions (e. g. Na +) and strong –ve ions (e. g. (Cl-) = strong ion difference (Stewart’s Theory) • Physiological strong ion difference ≈ 40 mmol/L (140 – 100) • 0. 9% Saline contains 154 mmol/L Na+ and 154 mmol/L Cl- • Chloride rises disproportionately to sodium reducing the strong ion gap and resulting in (hyperchloraemic) acidosis • Renal vasoconstriction and impaired secretion of sodium • Clinicians often respond to acidosis by giving more fluids… • Don’t forget, 0. 9% saline is also present in colloids e. g. HAS, Gelofusine®, Volplex®, Voluven® • Balanced colloids now available e. g. Gelaspan®, Isoplex®, Volulyte®
MYTHS ABOUT BALANCED CRYSTALLOIDS… ‘…but it’s got potassium in it…’ • Hyperchloraemia causes acidosis which exacerbates hyperkalaemia • Normal saline may raise [K+] more than balanced solutions in AKI O’Malley et al, Anesthesia and Analgesia, 2005 ‘…but it’s got lactate in it…’ • Lactate per se is not bad for you: it is a marker of disease severity • Lactate in Hartmann’s ≠ lactic acid; it is a conjugate base (potential HCO 3 -) and will NEVER increase acidosis • The patient will be making a lot more lactate (1500 mmol/d in health) than you will be giving therefore effect on total body lactate negligible
THE GREAT FLUID DEBATE CONTINUES… Balanced vs non-balanced crystalloids • 0. 9% Saline slightly cheaper than Hartmann’s (£ 0. 78/L vs £ 1. 00/L) but is associated with hyperchloraemic acidosis: • Potential for renal vasoconstriction (AKI and hyperkalaemia), impaired GI perfusion and coagulopathy • Relevance in terms of clinical outcomes uncertain (large trials on-going) Crystalloids vs colloids • Equivalent patient outcomes in most studies • Colloids associated with greater expense, risk of anaphylaxis, coagulopathy and increased risk of AKI (especially starches - withdrawn) • Albumin probably reasonable choice in sepsis?
FLUID THERAPY: BACK TO BASICS Restore circulating volume • Diagnosis and treatment of hypovolaemia Correct dehydration • Reduced total body water with preservation of circulating volume Maintain circulating volume and electrolytes • Understand anticipate physiological requirements
RECOGNIZING & TREATING HYPOVOLAEMIA Treating Hypotension Hypovolaemia 1. Vital signs and MEWS Tachycardia Record patient observations Central Pressure Urine Venous output (Oliguria) Tachypnoea 2. Diagnostic tests 3. CVP and oliguria 4. The fluid challenge Choose your weapon! Cannot describe euvolaemia Does not. Delayed ‘diagnose’ hypovolaemia capillary refill Give 500 m. L QUICKLY (≤ 15 mins) Is. Oliguria no longer recommended as a should trigger a volume Cool peripheries Stayresuscitation by theraise patient and repeat Passive leg test assessment, NOT a target fluid challenge observations Autotransfusion 500 m. L of blood Other (less of invasive) means of from ‘guiding’ Oliguria may indicate dehydration Repeat until patient no longer legs boluses and fluidabdomen resuscitation hypovolaemic Urine output is not a good target in the Effect maximal at 30 -90 s Helpful at extremes ofpatient filling only acutely unwell If no haemodynamic response after 2 L of fluid (i. e. –veand/or test) contact Critical 10% increase in s. BP reduction in Care HR predictive of fluid responsiveness > POLL
GETTING IT WRONG… Dry Wet Over-transfusion: ‘fluid in the wrong place’ • Pulmonary oedema, gut oedema, peripheral oedema, anasarca • Capillary injury and shedding of EGL Dry Wet Under-transfusion: hypoperfusion and persisting shock • AKI • Ischaemic hepatitis / colitis • Arrhythmias / ACS • Cerebrovascular events • Multi-organ failure
WET, DRY OR SOMEWHERE IN-BETWEEN? Dry (Restricted) Wet (Liberal)
GETTING IT RIGHT FOR MEDICAL PATIENTS… Dry (Restricted) Wet (Liberal) d i lu rg’ a f g n e i t n i ’ s t z h u e i c b n m a Frequentt. Reassessment is Key! i s o i o r t p r p a e O t ‘ sectit ap d u W e s ‘ t e r rge ta Dry Wet
MAINTENANCE FLUIDS Wet Dry 25 -30 m. L/kg/day 1 mmol/kg/day of Na+, Cl- and K+ 25 m. L/kg/day of: 0. 9% Na. Cl Hartmann’s 4% Glucose-0. 18% Saline + 40 KCl + > 4 mmol/kg/day Na Na 3. 3 mmol/kg/day > 0. 45 mmol/kg/day Na+ + > 4 mmol/kg/day Cl Cl. Cl-- 2. 8 mmol/kg/day > 0. 45 mmol/kg/day 0. 125 mmol/kg/day > 1 mmol/kg/day K+ K+ > 70 g glucose
REPLACEMENT One of the few indications for ‘normal’ saline
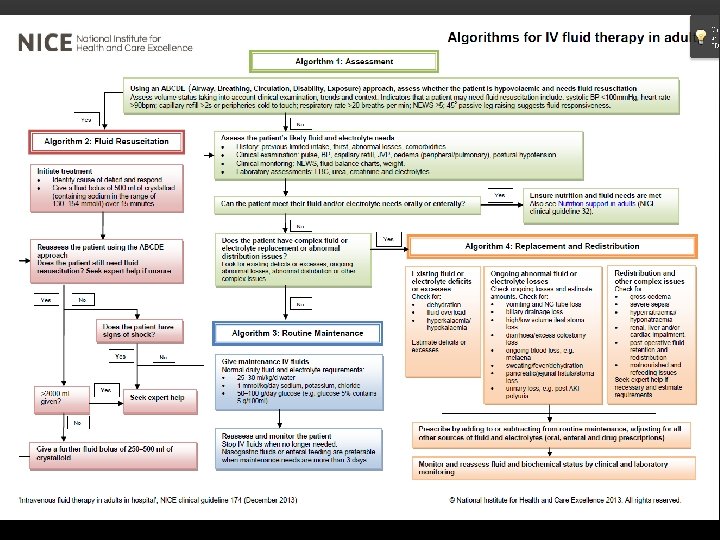
SUMMARY: 5 RS o t n i g n i k a t s n o i d t n p a i r s c e s s e s r o p l d g i n u i l f o t g n d e e n z o i m l , s a s s u u e t d s i a s v t i a s e r e Ind t m n u e l u o q v e t r n f accou ution with b i r t s i d re
DISCUSSION COMMENTS ? QUESTIONS