INTRAUTERINE GROWTH RESTRICTION IUGR Seluk zden MD Prof
 Selçuk Özden MD, Prof")


 • SGA: Small")


 <2500 g • Very Low Birth Weight")
: There is no structural anomaly; Doppler")



 2. Cellular hyperplasia +")



 ↓")



















 § BPD (Biparietal diameter),")

























- Slides: 62
INTRAUTERINE GROWTH RESTRICTION (IUGR) Selçuk Özden MD, Prof
INTRAUTERINE GROWTH RESTRICTION § IUGR, is the second most important cause of perinatal mortality after preterm delivery. § Perinatal mortality is increased 6 to 10 times (120/1000)
INTRAUTERINE GROWTH RESTRICTION § 53 percent of preterm stillbirths and, § 26 percent of term stillbirths § Intrapartum asphyxia is increased (50%) § It is possible to prevent prenatal complications by appropriate diagnosis and management.
FETAL GROWTH § AGA: Appropriate for gestational age (10 -90. p) • SGA: Small for gestational age (<10. p) • LGA: Large for gestational age (>90. p)
FETAL GROWTH § 1. characteristics
FETAL GROWTH § Fetal weight normogram according to gestational age. Lubchencho et al. 1. characteristics
DEFINITIONS § • Low Birth Weight (LBW) <2500 g • Very Low Birth Weight (VLBW) <1500 g • Extremely Low Birth weight (ELBW) <1000 g • Macrosomia >4000 g
TERMINOLOGY 1. Normal Small Fetuses: (Small Happy Babies): There is no structural anomaly; Doppler findings and amniotic fluid volume normal; fetal weight is low. These babies are not risky, and no need special care 2. Abnormal Small Fetuses- There is genetic or structural anomaly. Pregnancy termination is offered. 3. Intrauterine Growth Restriction (= IUGR)- Placental function is impaired. These fetuses need appropriate management and observation.
INTRAUTERINE GROWTH RESTRICTION § Cut-off values for diagnosis: § <10. th percentile § <5 th. percentile § Mean± 2 SD (3. th percentile)
INTRAUTERINE GROWTH RESTRICTION § Growth normograms are based on different ethnic and geographic regions.
§ Growth normograms are based on different ethnic and geographic regions
PHASES OF FETAL GROWTH 1. Cellular hyperplasia (first 16 weeks) 2. Cellular hyperplasia + hypertrophy (until 32. th weeks) 3. Cellular hypertrophy (after 32 weeks).
PHASES OF FETAL GROWTH § Impaired dynamics of fetal growth effects § number of cells, § size of cells or both and § cause abnormal fetal weight, body mass or body ratios
CLASSIFICATION of IUGR § Symmetric IUGR • Head and body of the baby are proportionately small • May be caused by an event during early pregnancy Asymmetric IUGR • Head of the baby is abnormally bigger than the body • May be caused by an event during late pregnancy
CLASSIFICATION of IUGR
SYMMETRIC IUGR § Baby is small proportionally § Early events (chemical, viral, chromosomal) ↓ § Size and number of cells are decreased ↓ § Size of head and body are small propotionately
ASYMMETRIC IUGR § 2/ 3 of the IUGR § Abdominal growth is disproportionately small. § Late pregnancy pathologies (e. g. Preeclampsia) effect primarily size of cell. § Hepatic storage ↓ → Abdominal circumference ↓ § Development of head and brain are not effected (brain sparing effect) § In severe cases, ratio of head circumference to abdominal circumference increase to 1/5
ASYMMETRIC IUGR § 20 percent of fetuses with IUGR, growth of head is asimetrical with respect to abdomen § Intrapartum and neonatal complications § However, adverse pregnancy outcomes are different from normal fetuses
MORTALITY & MORBIDITY § Fetal dead, asphyxia, meconium aspiration, neonatal hypoglycemia and hypothermia ↑ § Abnormal neurologic development ↑ § Preterm IUGR de long-term mortalite ↑
ACCELERATION OF MATURATION § Lung maturation is accelerated in IUGR. § Adrenal glucocorticoid secretion is increased in response to stress § Babies with IUGR has no advantage than preterm babies
ETIOLOGY of IUGR 1. General – Ethnicity, small parents, fetal gender. 2. Maternal causes 3. Fetal causes 4. Placental causes 5. Idiopathic- (40 percent of cases) – Cause ? – probably due to placental insufficiency.
ETIOLOGY of IUGR • Maternal Causes • Eating disorders • Chronic medical disorders • Vascular diseases • Hypertensive diseases of • • • pregnancy • Diabetic vasculopathies • Chronic renal diseases • Collagen vascular diseases • Thrombophilia • Antiphospholipid antibody synd. • These problems decreases uteroplacental blood flow Poor maternal nutrition Poor gestational weight gain Anemia High altitude Social deprivation Illicit drugs Cocaine Smoking Warfarine, hydantoine Maternal age >35
ETIOLOGY of IUGR • Fetal Causes • Constitutional • Multiple gestation • Aneuploidies (trisomi 13, 18, 21) • Congenital abnormalities • Diseases of cartilage and bone • Genetic syndromes • Infectious causes • Herpes, • Cytomegalovirus, • Rubella, • Toxoplasma gondii
ETIOLOGY of IUGR • Placental Causes • Single umbilical artery • Anormal placental development (1/3 of • Placental mosaisism cases) • Circumvallate plasenta, • Partial abruption, • Pl. Acrreta, • Placental infarcts, • Hemangioma • Placenta previa
FETAL AND MATERNAL EFFECTS of IUGR § The effects depend on the gestational week at the onset of placental insufficiency § If placental insufficiency start early, clinical feature is severe, and results in miscarriage or stillbirth
MATERNAL EFFECTS of IUGR • Resistance to placental blood flow increases • Active placental mass decreases
FETAL EFFECTS of IUGR § Appears early, § Nutrient flow to fetus decrease, § Glucose mobilize from the hepatic storage, § Physical findings of growth restriction appear, § Metabolic, endocrine, hematological, cardiovascular and behavioral manifestations appear depending on the duration and severity of placental insufficiency
FETAL EFFECTS of IUGR § Transfer of nutrients to fetus ↓ § Size of placenta and fetus ↓ § Fetal hypoglycemia § Gluconeogenesis from the hepatic storage § Transfer of amino acids ↓ § Breakdown of the muscle proteins § Oxidative metabolism ↓ → Lactat accumulation → Acidemia
FETAL EFFECTS of IUGR § Fetal hypoxia → erythropoietin secretion ↑ § Polycythemia → hemoglobin ↑ § Viscosity of blood ↑ § Placental dysfunction § Immune system is effected § Immunoglobulins, B-cell count, WBC ↓ § Risk of infectious complications ↑
FETAL EFFECTS of IUGR § Early fetal cardiovascular effects § Transport of nutrients by umbilical vein decrease, § Nutrient flow to vital organs increase, § Umbilical blood flow much more shunts to fetal hearth by ductus venosus
FETAL EFFECTS of IUGR § Resistance to blood flow of cerebral artery decrease § Blood flow to myocardium and brain increase § Decrease in renal perfusion result in oligohydramnios. § Fetal movements and breathing decrease
FETAL CIRCULATION §
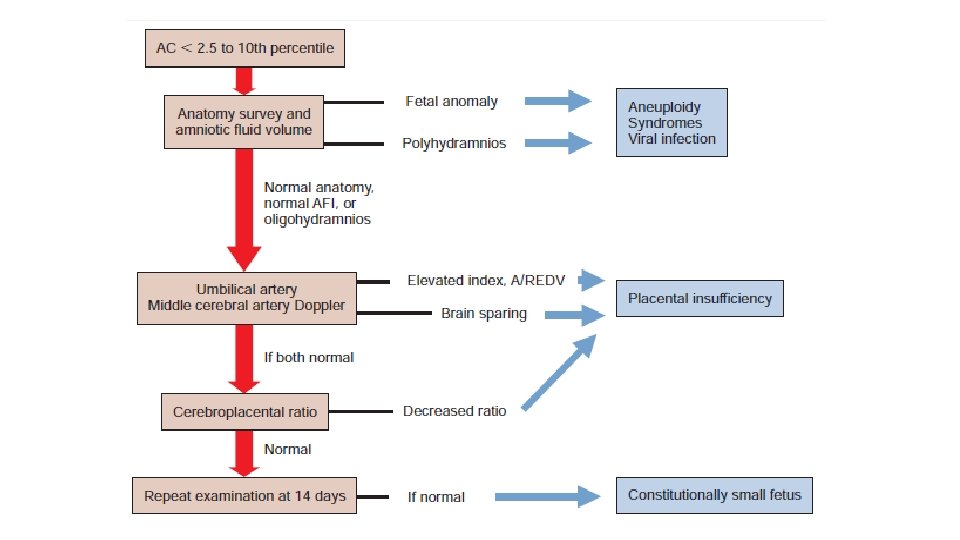
DIAGNOSIS of IUGR § Differential diagnosis: § Maternal diseases § Placental insufficiency § Aneupoidy and non-aneuploid syndromes § Viral infections.
DIAGNOSIS of IUGR § Determination of gestational age in early gestation, § Maternal weight gain, § Measurement of the symphysis-fundal height § Serial ultrasonography, § Definitive diagnosis may be impossible until delivery.
DIAGNOSIS of IUGR § Measurement of the symphysis-fundal height § Simple, cheaper, reliable § Able to diagnose 40 percent of cases. § Between 18 and 30 weeks’ gestation, the uterine fundal height in centimeters coincides within 2 weeks of gestational age. § If the measurement is more than 2 to 3 cm from the expected height, inappropriate fetal growth is suspected.
DIAGNOSIS of IUGR-ULTRASONOGRAPHY § Fetal biometry: § CRL (Crown-rump length) § BPD (Biparietal diameter), HC (Head circumference), TCD (Trans cerebellar Diameter) § Serial AC (Abdominal circumference) measurement in two week interval is the most invaluable measurement (<10 p). § Sonography fetal weight estimation § Ultrasound is not able to diagnose 30 percent of cases.
DIAGNOSIS of IUGR-ULTRASONOGRAPHY § §
DIAGNOSIS of IUGR-ULTRASONOGRAPHY § Initial sonography examination—usually at 16 to 20 weeks’ gestation establishes gestational age and identify anomalies. § Anatomical defects, markers of aneuploidies and non-aneuploid syndromes are detected by ultrasonography § Combining head, abdomen, and femur dimensions has been shown to optimize accuracy § Fetal growth is evaluated by repeat sonography evaluation at 32 to 34 weeks
DIAGNOSIS of IUGR-ULTRASONOGRAPHY § Amniotic Fluid Volume measurement: § Hypoxia and diminished renal blood flow has been hypothesized as an explanation for oligohydramnios. § Oligohydramnios increases prenatal mortality. § Single vertical pocket > 2 cm is normal, <1 cm ↓(oligohydramnios) § Four quadrant amniotic Fluid index (AFI) <5 cm ↓ (oligohidramnios)
DOPPLER VELOCIMETRY § Is both diagnostic and observation method § Fetal arterial and venous blood flow is evaluated. § Arterial Doppler: vascular resistance is evaluated § Blood flow velocity Waveform is evaluated by: § Ratio of Systolic/Diastolic velocities (S/D), § Resistance index (RI) and § Pulsatility index (PI)
DOPPLER VELOCIMETRY § Umbilical artery Doppler velocimetry: § As resistance to flow increase, end-diastolic flow decreases and disappears (absent end-diastolic flow) § Reversed arterial flow during diastole (negative S/D ratio) is an ominous sign that may precede fetal demise.
DOPPLER VELOCIMETRY • Normal Early diastolic notch
DOPPLER VELOCIMETRY § Other vessels: • Doppler of Ductus venosus • Middle cerebral artery • Abdominal aorta • Renal artery
MANAGEMENT § If fetal-growth restriction is suspected, then efforts are made § to confirm the diagnosis, § To assess fetal condition, and § To search for possible causes.
MANAGEMENT • If there is a strong suspicion of fetal anomalies, patient counseling and prenatal diagnostic testing are indicated • The timing of delivery is crucial, and the risks of fetal death versus the hazards of preterm delivery must be considered.
MANAGEMENT § Important factors for management 1. Gestational age and fetal maturity 2. Basic pathology and associated medical pathologies 3. Type of IUGR 4. Presence of congenital defects 5. Oligohydramnios 6. Results of fetal surveillance tests: (Echography, CTG, acoustic stimulation test, fetal movements, umbilical Doppler, fetal hemodynamic pattern, biophysical profile, etc)
PREVENTION OF IUGR § Important factors for management 1. Primary prevention 2. Secondary prevention 3. Tertiary prevention
PRIMARY PREVENTION § Primary prevention is applied during periconceptional period: § Smoking cessation, § Counseling about Toxoplasmosis, § Vaccination to prevent Rubella, § Early diagnosis of associated abnormalities § Prevention of multiple gestation during ART § Preventive strategies to prevent IUGR associated preeclampsia (contact to sperm, prevention of obesity and insuline resistance)
SECONDARY PREVENTION § Aim is to detect and treat the disease during preclinical period • Maternal serum screenings are disappointing: Increased AFP and h. CG accompanies IUGR, but are poor screening tests. • Increased Uterine artery resistance : plays a significant role in the management.
TERTIARY PREVENTION § Aim is to decrease fetal mortality and morbidity: 1. Therapeutic strategies, 2. Timing of delivery
THERAPEUTIC STRATEGIES § Nutritional supplementation § Asetyl salisilic acid, dipridamole § Bed rest § Sex steroids § Dextrose and amino acid perfusion § Atrial natriuretic peptid § Maternal hemodilution § Intra amniotic therapy § Beta mimetics § Giving nutrient directly to fetus § Sedative agents § Nitric oxide liberators § Heparine and anticoagulants § Immunological treatments § Oxygen
THERAPEUTIC STRATEGIES § Therapeutic strategies are dissapointing § There is no specific treatment § Frequently, modified bed rest is offered
TIMING of DELIVERY § There is no definitive treatment of IUGR, § So, timing of delivery is important § Risks of prematurity must be balanced against to fetal risks. § After 24 to 28 weeks, neonatal mortality ↓ § After 32 weeks, morbidity ↓
TIMING of DELIVERY § Management of IUGR near term § Immediate delivery is the best approach, § If there is oligohydramniosis, delivery is recommended § If fetal heart rate is normal, vaginal delivery is preferable. § The fetus can not tolerate delivery, cesarean section is recommended.
TIMING of DELIVERY § Preterm IUGR >34 weeks: § If fetal growth stops, delivery is planned. § Fetal lung maturity is confirmed by amniocentesis § To accelerate fetal lung maturity, corticosteroid therapy is recommended.
TIMING of DELIVERY § Preterm IUGR <34 weeks: § If fetal anatomy and fetal tests are normal, observation is preferable. § If fetal growth progress and fetal test are normal, fetus is observed until fetal maturity § Fetal growth is evaluated by serial sonography
TIMING of DELIVERY § Between 27 -34 weeks: § If there is fetal risk, delivery may be planned. § To accelerate fetal lung maturity, corticosteroid therapy is recommended § Between 24 -27 weeks: § Fetus is immature during this period. § Perinatal mortality is 50% § So, maternal condition is the most important to choose interventions (e. g: preeclampsia)
LABOR AND DELIVERY § Oligohydramnios causes compression of umbilical cord § Fetus must be observed closely in the intrapartum period. § Rate of cesarean delivery ↑ § Fetal hypoxia and meconium aspiration ↑ § Staff proficient in resuscitative techniques must be available.
LABOR AND DELIVERY § Conditions Requiring Birth 1. If fetal growth does not progress during 3 weeks period. 2. Oligohydramnios 3. Abnormal venous Doppler, reverse diastolic flow in umbilical artery , low score of biophysical profile, or deceleration in cardiotocography 4. Disorders of acid-base balance in fetal blood drawn by cordocentesis
ROUTE of DELIVERY § Two of 3 fetus with IUGR are able to tolerate vaginal delivery • Rate of cesarean delivery: 30 -50% • Decision about labor induction or cesarean depends on: • Conditions of the fetus, • Special obstetric characteristics (Parity, presentation, cervical ripening)
REFERENCES 1. Williams Obstetrics 24. th edition-Cunningham et al. The Mc. Graw-Hill Companies-2014 2. Gabbe: Obstetrics: Normal and Problem Pregnancies, 6 th ed. , 2013 3. Current Obstetrics & Gyneacology , Mc. Graw. Hill, LANGE, 12 th edition 2015