Intracellular Accumulation Hussam Telfah MBBS FRCPath General points

Intracellular Accumulation Hussam Telfah, MBBS, FRCPath

General points • A manifestation of metabolic derangements is intracellular accumulation of abnormal amounts of various substances. • Types: A- Normal cellular components B- Abnormal substances • • Exogenous Endogenous Transient or permanent Harmless or toxic Cytoplasmic, within organelles or nuclear Can be reversible or progressive leading to death
. •")
Mechanisms • Inadequate removal of normal endogenous substance (defects in packaging and transport). • Accumulation of abnormal endogenous substance due to defects in folding, packaging, transport or secretion. • Normal endogenous substance accumulation due to defects in metabolism (degrading) enzymes. • Abnormal exogenous substance accumulation due to absence of degrading or transporting mechanisms.

Fatty change, Antitrypsin deficiency, CNS degenerative disorders Storage diseases Carbon and silica

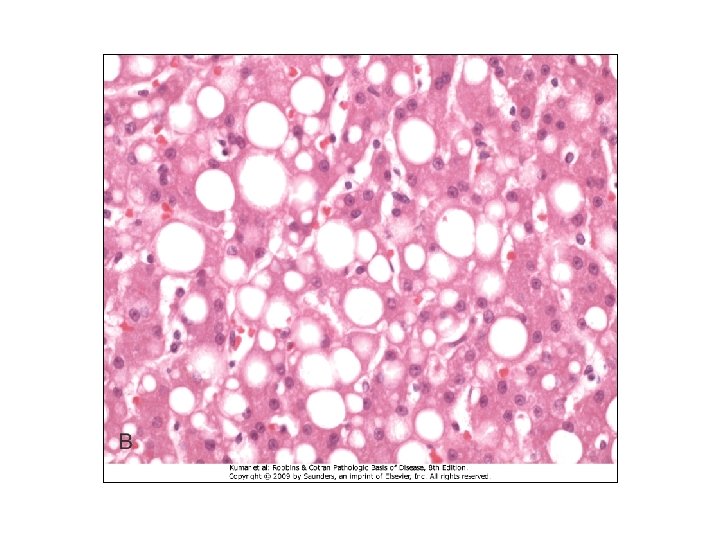
Lipids • All major classes of lipids can accumulate in cells. • Steatosis (Fatty change): triglycerides in parenchymal cells. • Mainly liver but, heart, muscle and kidney also. • Causes: toxins (alcohol), protein malnutrition, DM, obesity and anoxia.
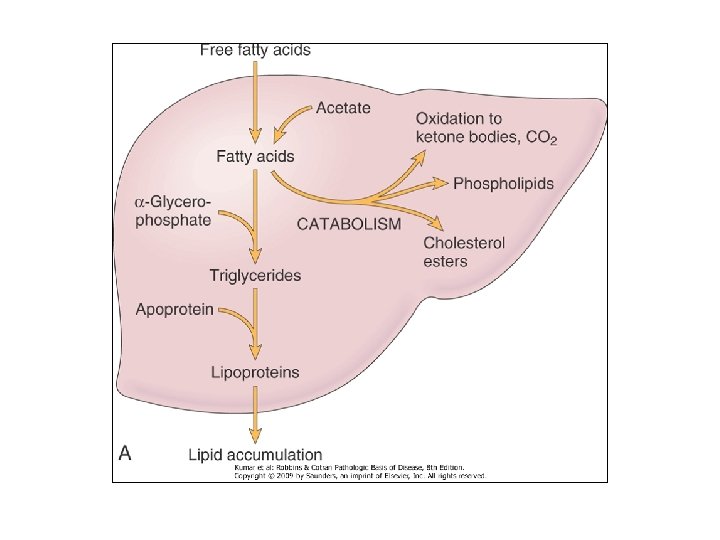

• Alcohol increases synthesis and decreases breakdown of lipids. • Protein malnutrition and CCL 4 reduce synthesis of apoproteins. • Hypoxia inhibits fatty acid oxidation • Starvation increases fatty acid mobilization from peripheral stores. • Consequences.

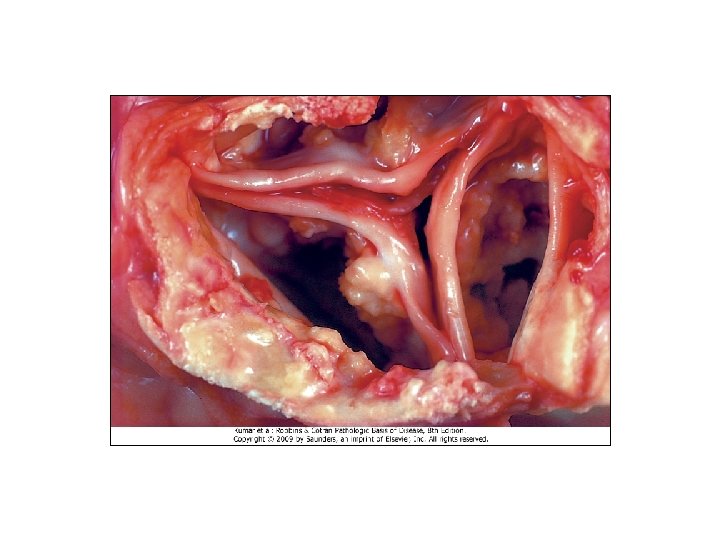
• Cholesterol & cholesterol esters • Atherosclerosis, xanthomas, cholesterolosis

Proteins • Less common than lipids. • Appears rounded eosinophilic droplets, vacuoles or aggregates. • Reabsorption of protein in renal tubules.

• Excessive production of proteins. Igs in plasma cells. Russell bodies.

• Defective intracellular transport and secretion of critical proteins. Antitrypsin deficiency.

• Accumulation of cytoskeleton proteins. • Intermediate filaments : keratin, neurofilaments, desmin, vimentin, glial. • Alcoholic hyaline (Mallory body), neurofibrillary tangle.

Hyaline change • Descriptive rather than specific marker for cell injury.

Glycogen • Glycogen storage diseases • DM
 Anthracosis, Tattooing • Endogenous: Lipofuscin, brown atrophy.")
Pigments • Exogenous: Carbon (coal dust) Anthracosis, Tattooing • Endogenous: Lipofuscin, brown atrophy.

Pigments • Melanin • Hemosiderin

Pathologic calcification • Abnormal deposition of calcium salts in tissues. • Dystrophic vs metastatic. • Dystrophic: in dying and necrotic tissues. Normal calcium levels. • H&E basophilic granular material. Can be intra - or extracellular. Heterotopic bone may develop. Psammoma bodies.
 and propagation then formation of crystalline calcium phosphate.")
• Pathogenesis: • Initiation (nucleation) and propagation then formation of crystalline calcium phosphate. • Calcium is concentrated in membrane bound vesicles. • Calcium concentrated in vesicles due to its affinity to membrane phospholipids. • Phosphates accumulate due to phosphatases

• Metastatic calcification: normal tissues. Hypercacemic status. • Causes: hyperparathyroidism, destruction of bone, vitamin. D related disorders and renal failure. • Affects tissues throughout the body. Mainly affects the interstitial tissues of gastric mucosa, kidneys, lungs, systemic arteries and pulmonary veins.

Cellular aging • Progressive decline in the proliferative capacity and life span of cells and the effects of continuous exposure to exogenous factors that cause accumulation of cellular and molecular damage. Mechanisms: • DNA damage. Accumulation of damaged DNA. Some aging syndromes are associated with defects in DNA repair mechanisms.

Cellular aging • Decreased cellular replication. Replicative senescence. Telomere shortening and cell cycle arrest. Enzyme telomerase (germ and stem cells) maintains the length of these telomeres. • Defective protein homeostasis. • Accumulation of metabolic damage. Reactive oxygen species

Cellular aging • Calorie restriction and environmental stresses alter signaling pathways that influence aging. • Decreased insulin/GF signaling, reduced activation of kinases and promotion of Sir 2 counteracts aging.
- Slides: 24