INTESTINAL OBSTRUCTION TYPES OF INTESTINAL OBSTRUCTION DYNAMIC where

INTESTINAL OBSTRUCTION

TYPES OF INTESTINAL OBSTRUCTION DYNAMIC – where peristalsis is working against a mechanical obstruction. ADYNAMIC – where mechanical element is absent. 1. Peristalsis may be absent; eg: paralytic ileus 2. Peristalsis present in a non propulsive form. Eg : mesenteric vascular occlusion

Clinical classification HIGH LOW
 ACUTE OBSTRUCTION CHRONIC OBSTRUCTION ACUTE ON CHRONIC OBSTRUCTION SUBACUTE OBSTRUCTION")
CLASSIFICATION (Contd. . ) ACUTE OBSTRUCTION CHRONIC OBSTRUCTION ACUTE ON CHRONIC OBSTRUCTION SUBACUTE OBSTRUCTION

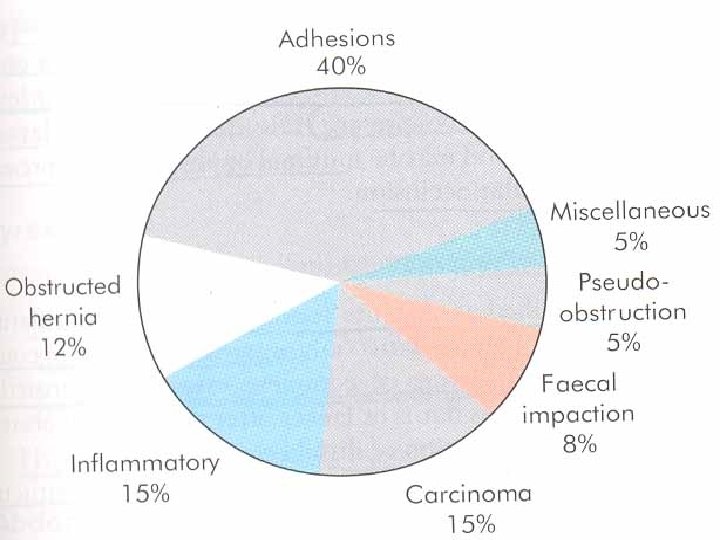
CAUSES OF INTESTINAL OBSTRUCTION

DYNAMIC INTRALUMINAL impaction foreign bodies bezoar gall stones INTRAMURAL strictures malignancy EXTRAMURAL bands/adhesions hernia volvulus intussusception ADYNAMIC paralytic ileus mesenteric vascular occlusion pseudo obstruction

PATHOPHYSIOLOGY ABOVE THE LEVEL OF OBSTRUCTION Obstruction proximal peristalsis is increased proportional to the distance of obstruction Obstruction not relieved bowel begins to dilate reduction in peristaltic strength flaccidity & paralysis
 FLUID (digestive juices)")
PATHO PHYSIOLOGY Distension proximal to obstruction GAS (nitrogen & hydrogen sulphide) FLUID (digestive juices) BELOW THE LEVEL OF OBSTRUCTION Normal peristalsis & absorption till empty then bowel contracts and becomes immobile

STRANGULATION Venous return is compromised increase in capillary pressure local mural distension loss of intravascular fluid & RBCs occurs Once the arterial supply is impaired, hemorrhagic infarction occurs viability of the bowel wall is compromised translocation & systemic exposure to aerobic & anaerobic organisms with their toxins.

CAUSES OF STRANGULATION EXTERNAL hernial orifices adhesions/bands INTERRUPTED BLOOD SUPPLY volvulus, intussusception INCREASED INTRALUMINAL PRESSURE closed loop obstruction PRIMARY mesenteric infarction

CLOSED LOOP OBSTRUCTION Occurs when the bowel is obstructed at both the proximal & distal points. There is no early distension of the proximal intestine. When gangrene of the strangulated segment occurs, retrograde thrombosis of mesentric veins results in distension on both sides.

ACUTE INTESTINAL OBSTRUCTION CARDINAL FEATURES Abdominal pain Distension Vomiting Absolute constipation Visible peristalsis

CONDITIONS WHERE CONSTIPATION IS NOT SEEN Richter’s hernia Gallstone obturation Mesenteric vascular occlusion. Obstruction associated with pelvic abscess Partial obstruction

OTHER MANIFESTATIONS DEHYDRATION HYPOKALAEMIA PYREXIA – may indicate 1. onset of ischemia 2. intestinal perforation 3. associated inflammation HYPOTHERMIA ABDOMINAL TENDERNESS

Clinical features of strangulation Presence of shock indicates underlying ischemia Constant pain Symptoms usually commence suddenly & recur regularly Localised tenderness will always be present associated with rigidity/rebound tenderness

INTERNAL HERNIA SITES OF INTERNAL HERNIA foramen of winslow Defect in the mesentery Defect in the transverse colon Defects in the broad ligament Congenital or acquired diaphragmatic hernias, Duodenal retro perironeal fossae Caecal/ appendiceal retroperitoneal fossae Inter sigmoid fossa

OBSTRUCTION FROM ENTERIC STRICTURES Occurs secondary to TB or Crohn’s disease Malignant strictures lymphoma Presentation is sub a/c or c/c Standard surgical management is resection& anastomosis Strictureplasty for Crohn’s

BOLUS OBSTRUCTION FOOD GALL STONES TRICHO BEZOARS PHYTO BEZOARS STERCOLITHS WORMS

TRICHO BEZOAR STERCOLITH FABRIC BEZOAR

ACUTE INTUSSUSCEPTION Occurs most commonly in children, in an idiopathic form peak incidence at 3— 9 months. hyperplasia of Peyer’s patches in the terminal ileum may be the initiating event secondary to weaning. adenovirus or rotavirusis also assosciated.

OLDER CHILDREN Meckels diverticulum polyp duplication HSP ADULTS Polyp Sub mucosal lipoma tumour

ACUTE INTUSSUSCEPTION This occurs when one portion of the gut becomes invaginated within an immediately adjacent segment; invariably it is the proximal into distal bowel.

Contd… Three parts Entering or inner tube Returning or middle tube Sheath or outer tube (intussuscipiens)

APEX The part which advances MASS is the intussusception NECK is the junction of the entering layer with the mass

CLINICAL FEATURES An otherwise fit and well male child of 6 months develops sudden onset of screaming associated with drawing up of the legs. The attacks last for a few minutes, recur every 15 minutes and become progressively severe. During attacks the child has facial pallor whilst between episodes he is listless and drawn.

Contd… Vomiting may or may not occur but ‘red current’ jelly stool is characteristic Abdomen is not distended, a lump may be felt. Emptiness in the right iliac fossa (the sign of Dance). On rectal examination blood stained mucus may be found on the finger.

RADIOGRAPHY OF ACUTE INTUSSUSCEPTION PLAIN ABDOMINAL FILM Absent caecal gas shadow BARIUM ENEMA Claw sign

Supine and crosstable lateral views demonstrating findings consistent with iliocolic intussusception.

BARIUM ENEMA Showing CLAW SIGN

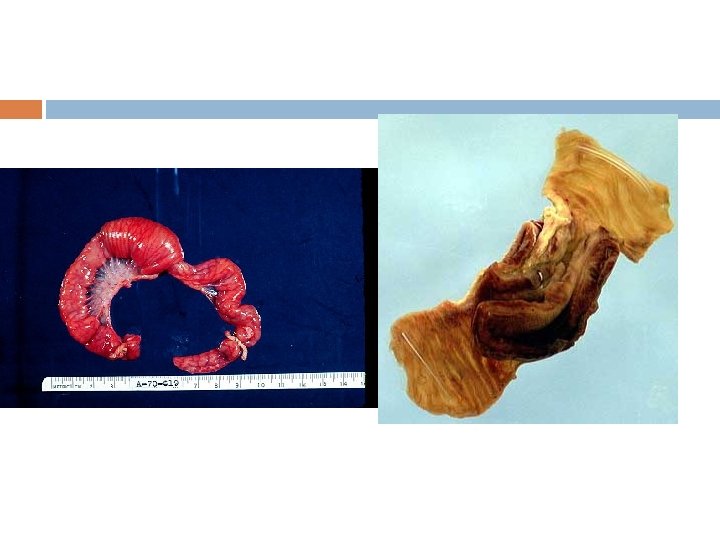
INTUSSUSCEPTION ON A MECKELS
 associated with a characteristic rash and abdominal")
DIFFERENTIAL DIAGNOSIS Acute enterocolitis Henoch—Schönlein purpura (HSP) associated with a characteristic rash and abdominal pain Rectal prolapse

MANAGEMENT Operative management is required where hydrostatic reduction has failed or is contraindicated After complete preoperative resuscitation laparotomy & reduction

In the presence of an irreducible or gangrenous intussusception the mass should be excised in situ and an anastomosis or temporary end stoma created. Adequate postoperative care

VOLVULUS OF THE SMALL INTESTINE This may be primary or secondary Usually occurs in the lower ileum.


It may occur spontaneously following consumption of a large volume of vegetable matter or secondary to adhesions Treatment consists of reduction of the twist and is then directed to any underlying cause

VOLVULUS OF SMALL INTESTINE

COMPOUND VOLVULUS A rare condition also known as ileo sigmoid knotting. The long pelvic mesocolon allows the ileum to twist around the sigmoid colon resulting in gangrene The patient presents with acute intestinal obstruction, distension is mild.

Plain radiography reveals distended ileal loops in a distended sigmoid colon. Decompression, resection and anastomosis are required

ACUTE INTESTINAL OBSTRUCTION IN NEW BORN CONGENITAL ATRESIAS&STENOS IS VOLVULUS NEONATORUM MECONIUM ILEUS

CONGENITAL ATRESIA The incidence of atresia at different anatomical site Duodenum — 35 per cent Jejunum — 15 per cent Ileum — 25 per cent Ascending colon — 10 per cent Multiple sites — 15 per cent.

ATRESIA / STENOSIS OF THE DUODENUM A result of an intrauterine vascular accident Persistent vomiting occurs from birth with or without bile. Visible peristalsis may be seen in the left upper quadrant. Site at the level of the ampulla of Vater. 30% Down’s syndrome.

Radiography reveals a double stomach appearance Duodenal obstruction in infancy may also be due to midgut volvulus, a band obstruction or an annular pancreas Duodeno jejunostomy / A Witzel gastrostomy

OTHER ATRESIAS In ileal atresia abdominal distensionoccurs In jejunal atresia vomiting occurs early. Surgery. Secondary closure by circumstomal mobilization and anastomosis.

ARRESTED ROTATION Four major types of arrest. The whole bowel may remain free as a narrow based mesentery. The caecum may he displaced with transduodenal bands. The intestine may return in a clockwise direction A failure of rotation altogether

Clinical features are identical to duodenal stenosis Early laparotomy

MECONIUM ILEUS Neonatal manifestation of cystic fibrosis. Inspissated meconium may be palpated as a rubbery swelling. Abdominal radiography may reveal a distended small intestine, with mottling. Family history may be present


Complications such as volvulus neonatorum, atresia or meconium peritonitis can occur. If conservative management fails, laporotomy is indicated. The standard treatment is resection of the most dilated segment with an end to side anastomosis of the colon to the ileum. The distal ileal opening is formed into an ileostomy

NECROTISING ENTEROCOLITIS Seen in sick premature infants associated with hypoxia, hypothermia, hypotension and umbilical artery cannulation. The ileum, caecum are affected with a complete spectrum from mucosal to transmural necrosis.

Bilious vomiting, abdominal distension, colour change occurs Abdominal radiographs may show pneumatosis intestinalis. Laparotomy excision of all necrotic bowel with primary anastomosis is usual

CHRONIC INTESTINAL OBSTRUCTION The causes of obstruction may be ORGANIC Intramural faecal impaction Mural diverticulitis, strictures, anastomotic stenosis Extramural adhesion , metastatic deposits, endometriosis FUNCTIONAL pseudo obstruction. FUNCTIONAL

Constipation appears first. It is initially relative and then absolute Associated with distension and pain Vomiting is a late feature

Plain abdominal radiography may be useful. Contrast water soluble enema study to rule out functional disease. Organic disease requires a laparotomy Functional disease requires colonoscopic decompression and conservative management

ADYNAMIC OBSTRUCTION

PARALYTIC ILEUS It is a state in which there is failure of peristaltic waves secondary to neuromuscular failure Stasis accumulation of fluid and gas within the bowel with associated distension, vomiting, absence of bowel sounds and absolute constipation

TYPES OF PARALYTIC ILEUS Postoperative — self limiting with a duration of 24— 72 hours. Infection — intra abdominal sepsis Reflex ileus — fractures of the spine or ribs, retroperitoneal haemorrhage or application of a plaster jacket. Metabolic — uraemia and hypokalaemia.

CLINICAL FEATURES Occurs 72 hours after laparotomy No bowel sounds on auscultation No passage of flatus. Abdominal distension becomes more marked and tympanitic. Pain is not a feature. Radiologically, the abdomen shows gas filled loops of intestine with multiple fluid levels

MANAGEMENT Prevention by Nasogastric suction Restriction of oral intake Electrolyte balance must be maintained

General principles of specific treatment are The primary cause must be removed GI distension must be relieved by decompression Close attention to fluid and electrolyte balance Catchpole regime with neostigmine may be used in resistant cases If prolonged and threatens life laparotomy

SMALL BOWEL PSEUDO OBSTRUCTION Primary or secondary The clinical picture consists of recurrent subacute obstruction. The diagnosis is made by the exclusion of a mechanical cause. Treatment consists of initial correction of any underlying disorder. Cisapride is the drug of choice

RADIOLOGICAL DIAGNOSIS Obstructed small bowel is characterized by straight segments that are central and lie transversely. No gas is seen in colon Jejunum regularly spaced valvulae conniventes giving a concertina / ladder effect. Ileum featureless

At first gas shadows appear followed by fluid levels. Number of fluid levels is directly proportional to the degree of obstruction & to its site. Impacted foreign bodies and gas in gall stone ileus may also be visible in radiographs.

GAS FILLED LOOPS MULTIPLE FLUID LEVELS

PRINCIPLES OF TREATMENT OF ACUTE INTESTINAL OBSTRUCTION GASTROINTESTINAL DRAINAGE FLUID & ELECTROLYTE REPLACEMENT RELIEF OF OBSTRUCTION

SUPPORTIVE MANAGEMENT NASOGASTRIC DECOMPRESSION 4 th hourly aspiration by Ryle’s or Salem tube.

REPLACEMENT OF SODIUM AND WATER LOSS with Hartmann’s solution or normal saline. The volume required is determined by clinical, haematological & biochemical criteria. ANTIBIOTICS

SURGICAL TREATMENT INDICATIONS OF EARLY OPERATION Obstructed or strangulated external hernia Internal intestinal strangulation Acute obstruction

OPERATIVE ASSESSMENT SITE OF OBSTRUCTION NATURE OF THE OBSTRUCTION VIABILITY OF THE GUT

PRINCIPLES OF SURGICAL INTERVENTION MANAGEMENT OF SEGMENT AT SITE OF OBSTRUCTION DISTENDED PROXIMAL BOWEL UNDERLYING CAUSE OF OBSTRUCTION

STEPS OF SURGICAL PROCEDURES Identification & assessment of the caecum. Collapse indicates small bowel obstruction. Display the cause of obstruction by careful retrograde assessment. Operative decompression may be performed

Depending upon the nature of cause, enterolysis, excision, bypass or proximal decompression can be performed. Following relief of obstruction, viability of the involved bowel should be assessed
- Slides: 75