Interventions in Treating Patients With Low Back Pain

Interventions in Treating Patients With Low Back Pain

58 year old female Work: Inspects products Chief Complaint: L. LE Throbbing pain March, 2016 Pain Onset June, 2016 Steroidal Injections (Spaced a week apart) July, 2016 Starts PT

Tests and Measures: P-A Spring Testing: ü Mild Hypomobility ü Pain L 4 -S 1 Active Lumbar Ext. : ü Mild pain; 150 Active Lumbar Flex: ü Sharp pain; 450 SLR: ü 0 -350 caused pain (ipsilateral) Standing Lumbar Quadrant Ext. with Overpressure: ü +ive Myotomes: ü L. Knee Extension, L. ankle plantarflexion - 4/5 Slump Test: ü +ive

l e d o M F IC Body Structure and Function: Hypomobility Pain w/ Flex. • Hypomobility Pain w/ Ext. w/ Flex. • Pain Decreased Strength Health Condition: • Radiculopathy, lumbosacral region Participation: • Abilities: - sleep Sleep Able to through night • Restrictions: is painful -Work Spending time with Family - Family Driving - Driving Activity: Abilities: • Abilities: Standing to an extent - Standing Limitations: • Limitations: Sitting, putting shoes - Sitting on: • Pain w/ Ext. • Strength Environmental Factors +: +: Insurance Sufficient insurance Support from Family - : Stress of Work Personal. Factors Personal + : Motivated - : Stress about getting better so can work with no - : Stresspain
 Objective: To investigate prevalence and reliability of placement into a intervention")
(Physical Therapy, 2011) Objective: To investigate prevalence and reliability of placement into a intervention from translating the use of subgroups to a classification algorithm Study Design: • • Cross Sectional, Observational Study Test, Retest
")
(Physical Therapy, 2011)
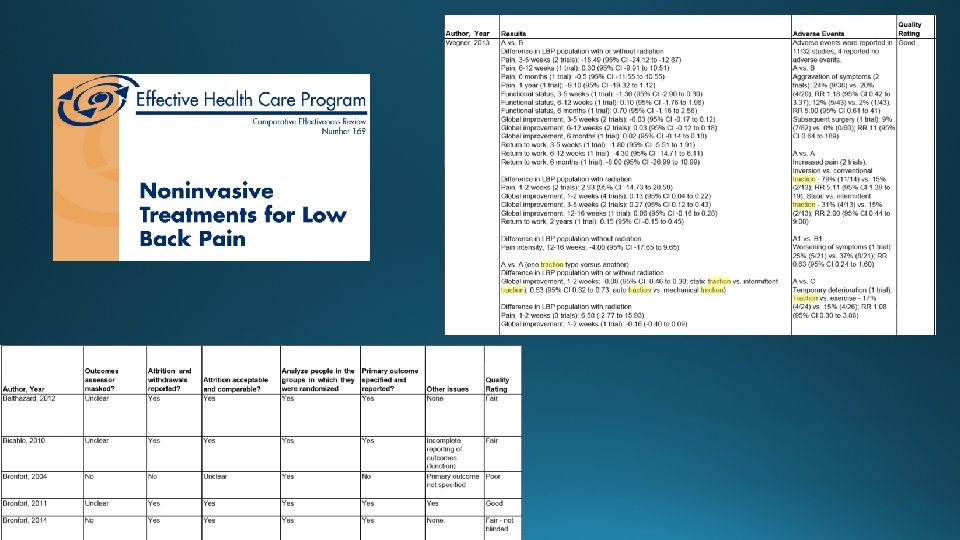
 Selection Criteria: RCT’s involving traction to treat acute,")
(Cochrane Database of Systematic Reviews, 2013) Selection Criteria: RCT’s involving traction to treat acute, subacute, or chronic nonspecific LBP w/ or w/0 sciatica (32 RCTs were included) Outcome Measurements: • Pain Intensity • Functional Status • Global Improvement • Return to Work *23/32 studies included mostly people with LBP and sciatica pain Results: • Low to moderate quality evidence - no impact on pain intensity, functional status, or global improvement Limitations: • Amount of high quality studies • Low to moderate quality evidence - makes little or no difference when comparing sham, placebo, or no treatment • 8 studies were a mix of with and without sciatic • 1 study had no sciatica pain • Studies distinguishing between people with different symptom patterns • Very low to moderate quality evidence - makes little or no difference when comparing physiotherapy and traction or other treatments Quality of Review: Good 2
 Objective: To compare spinal manipulative therapy (SMT) plus home")
(Annals of Internal Medicine, 2014) Objective: To compare spinal manipulative therapy (SMT) plus home exercise and advice (HEA) vs. HEA alone while studying the reduction in pain, short term and long term Study Design: • 192 patients (191 at 12 wks, 179 at 52 wks) • 96 patients assigned to each group • Patients were 21 y. o. or older and have had BRLP for at least 4 wks Limitations: • Patients and providers were not blinded • Study size • Back pain potentially gets better over time Outcomes: • Leg Pain • Low Back Pain • Global Improvement • Medication Use • Satisfaction
 (Annals")
*Effect size for leg pain at 12 wks was considered medium (0. 6) (Annals of Internal Medicine, 2014) Quality of Study: Fair 2

Why? The research I found does not compare traction and manipulation Clinical prediction rule for utilization of manipulation as an intervention for patients with LBP suggests less likelihood of success for patients with symptoms distal to the knee

Practicing at the top of Your License! Remember the 3 legged stool There is not one intervention for each diagnosis If something is not working, try something different Listen to your patients and figure out their goals to ultimately give them the best treatment

http: //www. apta. org/Media/Releases/Consumer/2012/4/4/
- Slides: 19