Interventions for nausea and vomiting in early pregnancy








 to assess eligible studies • Participants: Women experiencing nausea, vomiting or retching in")







- Slides: 18
Interventions for nausea and vomiting in early pregnancy: a Cochrane Review Clinical www. cochranejournalclub. com
Background • Can occur at any time of day • Most common in first trimester 6 -12/40, but can continue up to 20/40. • Persists beyond 20/40 in up to 20% • Associated with rising h. CG, • Hyperemesis gravidarum is severe and persistent vomiting, with weight loss >5%, dehydration and electrolyte imbalance, and affects 0. 3 -3% • Nausea and vomiting experienced by 50 -80%.
What Interventions?
Nice Guidelines: • • • Women should be informed that most cases of nausea and vomiting in pregnancy will resolve spontaneously within 16 to 20 weeks of gestation and that nausea and vomiting are not usually associated with a poor pregnancy outcome. If a woman requests or would like to consider treatment, the following interventions appear to be effective in reducing symptoms: • non-pharmacological – ginger – P 6 acupressure • pharmacological – antihistamines (no specific drug )
BWH Guidelines: – Reassurance – the condition is generally self-limiting and associated with a good prognosis – Dietary advice - adequate oral fluid intake to prevent dehydration, frequent small meals with high-carbohydrate or high-protein content (avoid offensive odours, fatty foods, spicy foods, iron supplements) – Oral anti-emetics if the patient's condition is unresponsive to oral fluids and dietary restrictions alone. Recommended first line drug is cyclizine 50 mg po tds and second line drugs include prochlorperazine 5 mg po tds, 3 -6 mg buccal bd or 25 mg od rectally, metoclopramide 10 mg po tds.
Clinical question What interventions are effective and safe for treating nausea and vomiting in early pregnancy? Source: Matthews A, Dowswell T, Haas DM, Doyle M, O’Mathúna DP. Interventions for nausea and vomiting in early pregnancy. Cochrane Database of Systematic Reviews 2010, Issue 9. Art. No. : CD 007575. DOI: 10. 1002/14651858. CD 007575. pub 2. www. cochranejournalclub. com 6
Context • This builds on a Cochrane review of interventions for nausea and vomiting in early pregnancy from 2003. www. cochranejournalclub. com 7
Methods • The Cochrane Pregnancy and Childbirth Group’s Trials Register was searched by the Trials Search Co-ordinator in May 2010. This Register contains reports of trials identified from: quarterly searches of the Cochrane Central Register of Controlled Trials (CENTRAL); weekly searches of MEDLINE; hand searches of 30 journals and the proceedings of major conferences; weekly current awareness alerts for a further 44 journals; and monthly Bio. Med Central email alerts. • The search identified 55 studies (in 66 reports). 27 of these studies were included and 22 were excluded. Four trials are awaiting further assessment and two trials are ongoing. • Outcomes are described approximately 3 days after the start of treatment. www. cochranejournalclub. com 8
PICO(S) to assess eligible studies • Participants: Women experiencing nausea, vomiting or retching in pregnancy, where recruitment to a trial took place up to 20 weeks’ gestation. (Women with the severe illness, hyperemesis gravidarum are excluded and covered in another review. ) • Intervention: All interventions for nausea, vomiting or retching. • Comparison: Any other intervention, including placebo and usual care. • Outcomes: Primary outcomes: symptomatic relief (measured as reduction or cessation of nausea, vomiting or retching), and adverse maternal and fetal/neonatal outcomes. Secondary outcomes: quality of life, and costs. • Studies: Randomized trials. (Cross-over and quasi-randomised studies were excluded. ) www. cochranejournalclub. com
Description of eligible studies • Twenty-seven trials were included, with a total of 4041 women. • Studies were found of the following comparisons: – Acupressure (P 6 point, including acustimulation and auricular) versus placebo or vitamin B 6 (7 studies, 795 women) – Acupuncture versus sham treatment and no treatment (2 studies, 648 women) – Moxibustion (Traditional Chinese Medicine) versus Chinese drugs (1 study, 302 women) – Ginger versus placebo, vitamin B 6 or drugs (9 studies, 1077 women) – Vitamin B 6 versus placebo (2 studies, 416 women) – Anti-emetic medications (6) versus placebo (6 studies with 803 women) www. cochranejournalclub. com
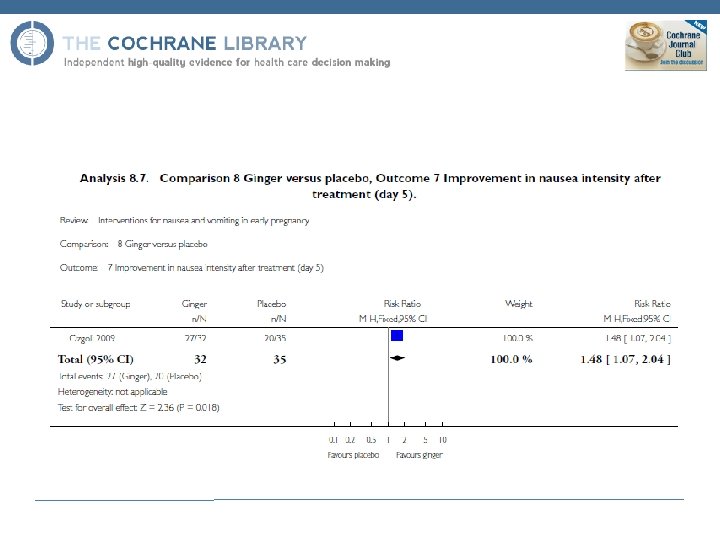
Results: symptom relief • No statistically significant difference between P 6 acupressure and placebo or vitamin B 6. • Results for auricular acupuncture difficult to interpret, and no statistically significant differences in the acupuncture study. • Improvements with both moxibustion and Chinese drugs, but this study is poorly reported. • Two studies favoured ginger over placebo • Some studies favoured ginger over vitamin B 6 and some favoured vitamin B 6 over ginger. • Vitamin B 6 was better than placebo. • Of the anti-emetic medications studied, the combination of dicyclomine (anti-cholinergic), doxylamine and pyridoxine was better than placebo. www. cochranejournalclub. com 12
Results: adverse effects and secondary outcomes • Adverse effects on the mother or baby Maternal effects – Side-effects from acupressure bands (both placebo and treatment groups) – Heartburn from ginger Fetal/neonatal effects – No studies found significant differences in adverse neonatal outcomes, but all were too small to detect any likely differences • Secondary outcomes – Quality of life was reported in few studies (and results were difficult to interpret) – No studies reported on economic costs www. cochranejournalclub. com 13
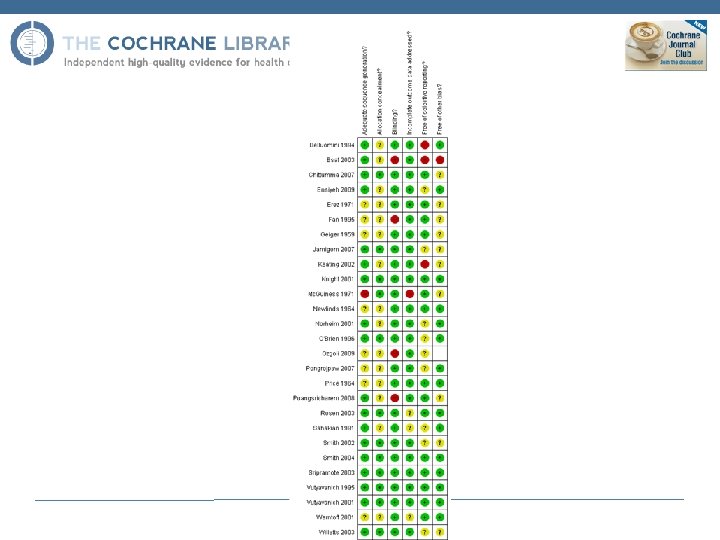
Conclusions: current evidence • There is little strong or consistent evidence for any intervention, and it is not possible to be confident in the effectiveness or safety of any of the interventions. • The methodological quality of studies was mixed, with inadequate information on randomisation procedures and blinding in many studies; and the results were difficult to interpret and pool because of differences in participants, interventions, comparisons and outcomes. • Some commonly recommended interventions, such as dietary and other behavioural advice, have not been studied. • No studies had the statistical power to provide convincing evidence of the effects on relatively rare adverse outcomes. • There was very little information on the psychological, social or economic effects of nausea and how these were affected by different interventions. www. cochranejournalclub. com 15
Limitations: • No research into cyclizine included • Limited research into prochlorperazine and metoclopramide ( Bsat 2003)
Conclusions: future research • There is a need for specific and justified outcomes in research on interventions for nausea and vomiting in pregnancy. • Several instruments have been used to measure outcomes and some of these might help address this (for example, the Pregnancy Unique Quantification of Emesis and Nausea (PUQE) scale). • Adherence to dietary and other advice should be measured consistently, because this may also affect symptom relief. • Adverse effects, quality of life and cost outcomes need to be collected and reported. www. cochranejournalclub. com 17
Useful links • Cochrane Journal Club discussion points • Interventions for nausea and vomiting in early pregnancy www. cochranejournalclub. com