Interventions for clients with oral cavity problems Interventions

Interventions for clients with oral cavity problems. Interventions for clients with esophageal disorders.

Mouth § Consists of lips and oral cavity-disorders can impact speech, nutritional intake and overall health. § Provides entrance and initial processing for nutrients and sensory data: taste, texture and temperature. § Salivary glands produce secretions containing ptyalin for starch digestion and mucus for lubrication § Pharynx aids in swallowing from mouth to esophagus.

Stomatitis Painful inflammation & ulceration of the mouth as a result of § § § Infection Vitamin deficiency Systemic disease Medications Trauma Food allergy Clinical findings vary by cause § Dry mouth § Ulcerations/lesions § Fissures § Bacterial or fungal growth § Pain § Odor

Stomatitis § Dry, painful mouth, open ulcerations, predisposing the client to infection § Commonly found on the buccal mucosa, soft palate, oropharyngeal mucosa, and lateral and ventral areas of the tongue § If candidiasis, white plaquelike lesions on the tongue; when wiped away, red sore tissue appears

Stomatitis Nursing Care § Frequent gentle mouth care § soft brush or toothette; brush if tolerated § Avoid commercial mouthwashes; rinse with saline, bicarbonate, or peroxide solutions § Medications if infectious cause: antifungals or antivirals § Pain management § Topical anesthethetics § Appropriate food selection
 § Antifungals")
Stomatitis § Antibiotics such as tetracycline syrup and minocycline (swish and swallow) § Antifungals such as nystatin oral suspension (swish and swallow) § Intravenous acyclovir for immunocompromised clients with herpes simplex stomatitis § Anti-inflammatory agents and immune modulators § Symptomatic topical agents such as gargle or mouthwash

Oral Tumors Pre Malignant Lesions § Leukoplakia § Erythroplakia Oral lesions that do not heal, especially in clients who smoke tobacco, use “snuff”, alcohol use, sun exposure § Slowly developing changes in the oral mucous membranes characterized by thickened, white, firmly attached patches that are slightly raised and sharply circumscribed. § Related to factors that cause oral mucous membrane irritation (i. e. poorly fitting dentures, smoking) § Cannot be removed when scraped unlike candidal infection § Most common oral lesion among adults


Erythroplakia § Red, velvety mucosal lesions on the surface of the oral mucosa § Higher degree of malignant transformation in erythroplakia than in leukoplakia § Commonly found on the floor of the mouth, tongue, palate, and mandibular mucosa § Erythroplakia is a general term for red, flat, or eroded velvety lesions that develop in the mouth. In this image, a squamous cell carcinoma is surrounded by a margin of erythroplakia.


Squamous Cell Carcinoma § Most common oral malignancy: can be found on the lips, tongue, buccal mucosa, and oropharynx § Highly associated with aging, tobacco use, and alcohol ingestion § Tumor, node, metastasis classification system for tumors of the lips and oral cavity

Basal Cell Carcinoma § Occurs primarily on the lips § Lesion is asymptomatic and resembles a raised scab; evolves into ulcer with a raised pearly border § Aggressively involves the skin of the face, but does not metastasize § Major etiologic factor is exposure to sunlight

Kaposi’s Sarcoma § Malignant lesion arising in blood vessels § Usually painless § Raised purple nodule or plaque § Found on the hard palate, gums, tongue, or tonsils § Most often associated with AIDS

Tumors of the Oral Cavity Nursing Assessment § History for risk factors, esp. alcohol, tobacco § Inspection of mouth for lesions § Palpation of submandibular nodes § Pain assessment Diagnosis § CT of head and neck § Biopsy of lesions

Treatment of Oral Cancer § Radiation therapy § Skin care § Mouth care § Nutrition Surgical Excision § Procedure depends on size & location of tumor, and presence of metastasis: simple excision of lesion to removal of tongue and part of mandible

Surgical Management § § § Preoperative care Operative procedure Postoperative care § Maintaining airway patency § Protecting the operative area § Relieving pain § Promoting nutrition

Nonsurgical Management § § § Airway management Cough management Aspiration precautions

Acute Sialadenitis § Inflammation of a salivary gland, caused by infectious agents, irradiation, or immunologic disorders § Interventions § § § Hydration Application of warm compresses Massage of the gland Use of saliva substitute Use of sialagogues

Salivary Gland Tumors § Relatively rare among oral tumors § Often associated with radiation of the head and neck areas § Assessment: ability to wrinkle brow, raise eyebrows, squeeze eyes shut, wrinkle nose, pucker lips, puff out cheeks, and grimace or smile § Treatment of choice: surgical excision of the parotid gland

Esophageal Disorders § § § § Gastroesophageal reflux disease Hiatal hernia Esophageal cancer Esophageal diverticula Esophageal strictures Achalasia Esophageal varices
 of")
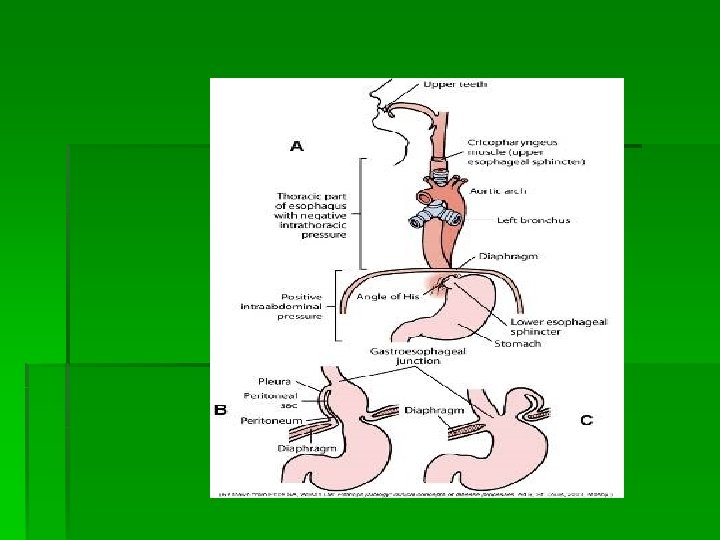
Gastroesophageal Reflux Disease § Occurs as a result of the backward flow (reflux) of gastrointestinal contents into the esophagus § Reflux esophagitis characterized by acute symptoms of inflammation § Esophageal reflux occurs when gastric volume or intra-abdominal pressure is elevated, the sphincter tone of the lower esophageal sphincter is decreased, or it is inappropriately relaxed.

Clinical Manifestations § § § Dyspepsia Regurgitation Hypersalivation or water brash Dysphagia and odynophagia Others manifestations: chronic cough, asthma, atypical chest pain, eructation (belching), flatulence, bloating, after eating, nausea and vomiting

Diagnostic Assessment § § § 24 -hr ambulatory p. H monitoring Endoscopy Esophageal manometry Esophagoscopy Indications and Contraindications. Indications include: § Dysphagia § Reflux § Hematemesis § Atypical chest pain § Many other conditions § Contraindications: § To assess reflux symptoms that respond to medical management § A uncomplicated sliding hiatal hernia

Nonsurgical Management § Diet therapy § Client education § Lifestyle changes: elevate head of bed 6 in. for sleep, sleep in left lateral decubitus position; stop smoking and alcohol consumption; reduce weight; wear nonbinding clothing; refrain from lifting heavy objects, straining, or working in a bent-over posture

Drug Therapy § Antacids elevate the level of the gastric contents. § Histamine receptor antagonists decrease acid production. § Proton pump inhibitors provide effective, long-acting inhibition of gastric acid secretion. § Prokinetic drugs increase gastric emptying and improve lower esophageal sphincter pressure and esophageal peristalsis.

Hiatal Hernia § Most common abnormality found of x-ray of upper GI § More common in older adults and in women

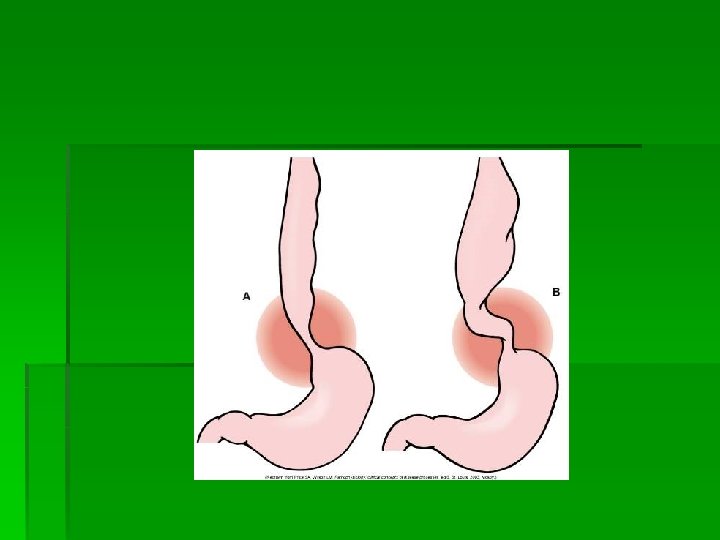
Hiatal Hernia § Protrusion of the stomach through the esophageal hiatus of the diaphragm into the thorax § Sliding hernia most common, occurring when esophagogastric junction and a portion of the fundus of the stomach slide upward through the esophageal hiatus into the thorax § Rolling hernia: fundus rolls into the thorax beside the esophagus

Assessment § § § Heartburn Regurgitation Pain Dysphagia Belching Worsening symptoms after eating or when in recumbent position

Nonsurgical Management § Drug therapy: antacids, histamine receptor antagonists § Diet therapy: avoid eating in the late evening and avoid foods associated with reflux § Weight reduction § Elevate head of bed 6 in. for sleep, remain upright for several hours after eating, avoid straining and vigorous exercise, avoid nonbinding clothing.

Surgical Management § § § Operative procedures Preoperative care Postoperative care § Respiratory care § Nasogastric tube management § Nutritional care for complications of surgery including gas bloat syndrome and aerophagia (air swallowing)

Achalasia § § § Rare, chronic disorder Affects 1 in 100, 000 Americans Affects all ages and both genders

Achalasia Etiology and Pathophysiology § Esophageal motility disorder believed to result from esophageal denervation characterized by chronic and progressive dysphagia § Primary symptoms: dysphagia and regurgitation of solids, liquids, or both

Achalasia Clinical Manifestations § Symptoms § Dysphagia § Most common symptom § Globus sensation § Substernal chest pain § During/after a meal § Halitosis § § Inability to belch GERD Regurgitation Weight loss

Achalasia Diagnostic Studies § § § Radiologic studies Manometric studies of lower esophagus Endoscopy

Drug and Diet Therapy § § § Calcium channel blockers Nitrates Direct injection of botulinum toxin into the lower esophageal muscle Semisoft foods Arching the back while swallowing Avoidance of restrictive clothing

Esophageal Dilation § Metal stents used to keep the esophagus open for longer durations § Complications: bleeding, signs of perforation, chest and shoulder pain, elevated temperature, subcutaneous emphysema, hemoptysis § Passage of progressively larger sizes of esophageal bougies using polyurethane balloons on a catheter

Esophagomyotomy § Surgical procedure for achalasia is done to facilitate the passage of food. § Laparoscopic approach is most common. § For long-term refractory achalasia, the surgeon may attempt excising the affected portion of the esophagus with or without replacement of a segment of colon or jejunum.

Esophageal Tumors § Esophageal tumors can be benign or malignant. § Barrett’s esophagus is ultimately malignant. § Clinical manifestations include dysphagia, odynophagia, regurgitation, vomiting, foul breath, chronic hiccups, pulmonary complications, chronic cough, and hoarseness.

Surgical Management § Esophagectomy: the removal of all or part of the esophagus § Esophagogastrostomy: the removal of part of the esophagus and proximal stomach § Minimally invasive esophagectomy § Extensive preoperative care § Operative procedures

Postoperative Care § Highest postoperative priority: respiratory care § Cardiovascular care § Wound management § Nasogastric tube management § Nutritional care § Discharge planning

Diverticula § Sacs resulting from the herniation of esophageal mucosa and submucosa into surrounding tissue § Zenker’s diverticulum most common § Diet therapy for size and frequency of meals § Surgical management

Diverticula

Esophageal Trauma § Trauma to the esophagus can result from blunt injuries, chemical burns, surgery or endoscopy, or stress of protracted vomiting. § Nothing is administered by mouth; broadspectrum antibiotics are given. § Surgical management requires resection of part of the esophagus with a gastric pullthrough and repositioning or replacement by a bowel segment.
- Slides: 45