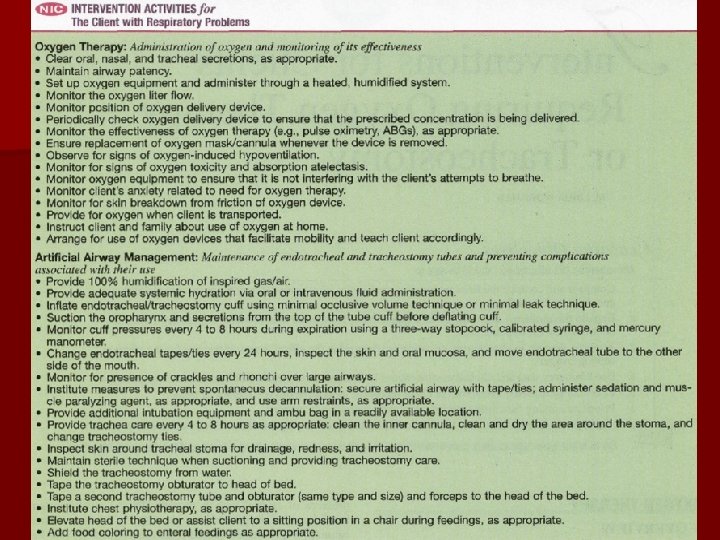
Interventions for Clients Requiring Oxygen Therapy or Tracheostomy











")


 is a newer technique using positive pressure to keep alveoli")
 is a long-term method of delivering oxygen directly")


















- Slides: 37
Interventions for Clients Requiring Oxygen Therapy or Tracheostomy
Therapeutic oxygen is used for both acute and chronic respiratory conditions associated with decreased blood and tissue oxygen levels as indicated by decreased partial pressure of arterial oxygen (Pa. O 2) levels or by decreased arterial oxygen saturation (Sa. O 2). n Conditions outside the respiratory system that increase oxygen demand, decrease oxygen-carrying capability of the blood, or decrease cardiac output also are indications for oxygen therapy. Such conditions include sepsis, fever, and decreased hemoglobin levels or poor hemoglobin quality n
The goal of oxygen therapy is to use the lowest fraction of inspired oxygen (Fi. O 2) to obtain the most acceptable oxygenation without causing the development of harmful side effects n The average client requires an oxygen flow of 2 to 4 L/min via nasal cannula or up to 40% via Venturi mask. n The client who is hypoxemic and also has chronic hypercarbia (increased partial pressure of arterial carbon dioxide [Pa. CO 2] levels) requires lower levels of oxygen delivery, usually 1 to 2 L/min via nasal cannula, to prevent decreased respiratory effort. (A low Pa. O 2 level is this client's primary drive for breathing. n
Hazards and Complications of Oxygen Therapy n n Combustion Oxygen-induced hypoventilation – The central chemoreceptors in the brain (medulla) are normally sensitive to increased Paco 2 levels, which stimulate breathing and cause an increased respiratory rate. When the Paco 2 increases over time to above 60 to 65 mm Hg, this normal mechanism shuts off. The central chemoreceptors lose their sensitivity to increased levels of Paco 2 and no longer respond by increasing the rate and depth of respiration, a condition called CO 2 narcosis. For these clients, the stimulus to breathe is a decreased arterial oxygen concentration as sensed by peripheral chemoreceptors found in the carotid sinus areas and aortic arch. When partial pressure of arterial oxygen (Pao 2) levels drop (hypoxemia), these receptors signal the brain to increase the respiratory rate and depth — the hypoxic drive to breathe. – The hypoxic drive occurs only in the presence of severely elevated Pa. CO 2 levels (i. e. , in the client who has hypoxemia and hypercarbia). When the client with low Pao 2 levels and high Paco 2 levels receives oxygen therapy, the Pao 2 level increases, removing the stimulation for breathing, and the client experiences respiratory depression. (The client being ventilated mechanically is not at risk for this complication.
Hazards and Complications of Oxygen Therapy n Oxygen toxicity n Absorption atelectasis n n Drying of the mucous membranes Infection – High concentrations of oxygen are avoided unless absolutely necessary. The addition of continuous positive airway pressure (CPAP) with an oxygen mask, bilevel positive airway pressure (Bi-PAP), or positive end-expiratory pressure (PEEP) on the mechanical ventilator may reduce the amount of oxygen needed. As soon as the client's clinical condition allows, the physician decreases the prescribed amount of oxygen – Nitrogen normally plays a large role in the maintenance of patent airways and alveoli. Making up 79% of room air, nitrogen prevents alveolar collapse. When high concentrations of oxygen are delivered, nitrogen is diluted, oxygen diffuses from the alveoli into the pulmonary circulation, and the alveoli collapse. Collapsed alveoli cause atelectasis (called absorption atelectasis), which is detected by auscultation
A bubble humidifier bottle used with oxygen therapy
Oxygen Delivery Systems n n n Oxygen delivery systems are classified according to the rate at which oxygen is delivered. There are two systems: low-flow systems and high-flow systems. Low-flow systems do not provide enough flow of oxygen to meet the total inspiratory effort of the client. Part of the tidal volume is supplied by inspiring room air. The total concentration of oxygen received depends on the respiratory rate and tidal volume. In contrast, high-flow systems provide a flow rate that is adequate to meet the entire inspiratory effort and tidal volume of the client regardless of the respiratory pattern. High-flow systems are used for critically ill clients and when it is particularly important to know the precise concentration of oxygen being delivered. If the client requires a mask but is able to eat, the nurse requests an order for a nasal cannula at an appropriate liter flow for mealtimes only. The mask is replaced after the meal is completed. To increase mobility, up to 50 feet of connecting tubing can be used with proper connecting pieces.
Low-flow oxygen delivery systems NASAL CANNULA. The nasal cannula, or nasal prongs, is used at flow rates of 1 to 6 L/min. Approximate oxygen concentrations of 24% (at 1 L/min) to 44% (at 6 L/min) can be achieved. n The nasal cannula is frequently used for chronic lung disease and for long-term maintenance of clients with other illnesses. The nurse places the nasal prongs in the nostrils, with the openings facing the client n
Low-flow oxygen delivery systems n SIMPLE FACE MASK. A simple face mask is used to deliver oxygen concentrations of 40% to 60% for short-term oxygen therapy or in an emergency. A minimum flow rate of 5 L/min is needed to prevent the rebreathing of exhaled air. The nurse gives special attention to skin care and to the proper fitting of the mask so that inspired oxygen concentration is maintained
Low-flow oxygen delivery systems PARTIAL REBREATHER MASK. A partial rebreather mask provides oxygen concentrations of 60% to 75%, with flow rates of 6 to 11 L/min. It consists of a mask with a reservoir bag but no flaps. The client first rebreathes one third of the exhaled tidal volume, which is high in oxygen, thus providing a high fraction of inspired oxygen (Fio 2). n The nurse ensures that the bag remains slightly inflated at the end of inspiration; otherwise, the client will not be getting the desired oxygen prescription. If needed, the nurse calls the respiratory therapist for assistance n
Low-flow oxygen delivery systems NON-REBREATHER MASK. A nonrebreather mask provides the highest concentration of the low-flow systems and can deliver an Fio 2 greater than 90%, depending on the client's breathing pattern. The non-rebreather mask is used most often with deteriorating respiratory status who might soon require intubation. n The non-rebreather mask has a oneway valve between the mask and the reservoir and two flaps over the exhalation ports. The valve allows the client to draw all needed oxygen from the reservoir bag, and the flaps prevent room air from entering through the exhalation ports. During exhalation, air leaves through these exhalation ports while the one-way valve prevents exhaled air from re-entering the reservoir bag. n
High-flow oxygen delivery systems n VENTURI MASK. The Venturi mask (commonly called Venti mask) delivers the most accurate oxygen concentration. Its operation is based on a mechanism that pulls in a specific proportional amount of room air for each liter flow of oxygen. An adaptor is located between the bottom of the mask and the oxygen source. Adaptors with holes of different sizes allow only specific amounts of air to mix with the oxygen. Precise delivery of oxygen results. Each adaptor also specifies the flow rate to be used; for example, to deliver 24% of oxygen, the flow rate must be 4 L/min. Another type of Venturi mask has one adaptor with a dial that the nurse uses to select the amount of oxygen desired. Humidification is not necessary with the Venturi mask. The Venturi system is best for the client with chronic lung disease because it delivers a precise oxygen concentration
High-flow oxygen delivery systems n n n OTHER HIGH-FLOW SYSTEMS. The face tent, aerosol mask, tracheostomy collar, and T-piece are often used to administer high humidity. A dial on the humidification source regulates the oxygen concentration being delivered. A face tent fits over the chin, with the top extending halfway across the face. The oxygen concentration varies, but the face tent, instead of a tight-fitting mask, is useful for facial trauma or burns. An aerosol mask is used when high humidity is required after extubation or upper airway surgery or for thick secretions. The tracheostomy collar can be used to deliver high humidity and the desired oxygen to the client with a tracheostomy. A special adaptor, called the T-piece, can be used to deliver any desired Fio 2 to the client with a tracheostomy, laryngectomy, or endotracheal tube. The flow rate is regulated so that the aerosol does not disappear on the exhalation side of the T-piece
A T-piece apparatus for attachment to an endotracheal or tracheostomy tube. Example of transtracheal oxygen delivery.
Noninvasive positive-pressure ventilation (NPPV) is a newer technique using positive pressure to keep alveoli open and improve gas exchange without the need for airway intubation. n This type of ventilation can deliver oxygen or may just use room air. Essentially, a nasal mask or full-face mask delivery system allows mechanical delivery of either bilevel positive airway pressure (Bi. PAP) or continuous nasal positive airway pressure. n For Bi. PAP, a cycling machine delivers a set inspiratory positive airway pressure each time the client begins to inspire. As the client begins to exhale, the machine delivers a lower set end expiratory pressure. Together, these two pressures improve tidal volume. n Nasal continuous positive airway pressure delivers a set positive airway pressure continually throughout each cycle of inhalation and exhalation. The effect is to open collapsed alveoli. Clients who might benefit from this form of oxygen or air delivery include those with postoperative atelectasis or cardiac-induced pulmonary edema. This technique is also used for sleep apnea. The effect of this use is to hold open the upper airways n
Transtracheal oxygen therapy Transtracheal oxygen (TTO) is a long-term method of delivering oxygen directly into the lungs. The physician passes a small, flexible catheter into the trachea via a small incision with the use of local anesthesia. n TTO allows better compliance and avoids the irritation that nasal prongs cause. Clients also report it to be more cosmetically acceptable. n A TTO team provides formal client education, including the purpose of TTO and care of the catheter. The physician prescribes a TTO flow rate for rest and for activity and a flow rate for the nasal cannula, to be used when the TTO catheter is being cleaned. The average client will have a 55% reduction in required oxygen flow at rest and a 30% decrease with activity n
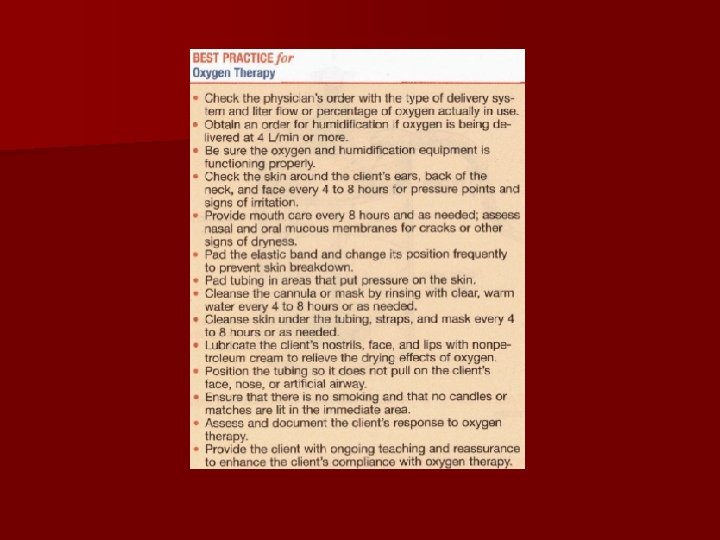
Home care management CRITERIA FOR HOME OXYGEN THERAPY n The client must be clinically stable and optimally treated before the need for home oxygen is considered. n For Medicare to cover the cost of continuous oxygen therapy, the client must have severe hypoxemia. n For reimbursement purposes, severe hypoxemia is generally defined as a partial pressure of arterial oxygen (Pao 2) level of less than 55 mm Hg or an arterial oxygen saturation (Sao 2) of less than 88% on room air and at rest. n The criteria are variable when hypoxemia is caused by cardiac rather than pulmonary problems, or when oxygen is needed only at night or with exercise
Home care management CLIENT EDUCATION n After the need for home oxygen therapy is verified, the nurse begins a teaching plan about oxygen therapy. The client, with the nurse's assistance, selects a durable medical equipment (DME) company to deliver oxygen equipment and a community health nursing agency for follow-up care in the home. The physician re-evaluates the need for oxygen therapy approximately 6 months after discharge from the health care facility and yearly thereafter. n While providing discharge planning and teaching, the nurse is sensitive to the client's psychologic adjustment to oxygen therapy. The nurse encourages the client to share feelings and concerns. The client may be concerned about social acceptance and misconceptions of friends. The nurse helps him or her realize that compliance with oxygen therapy is important so that normal activities of daily living (ADLs) and events that bring enjoyment can be continued
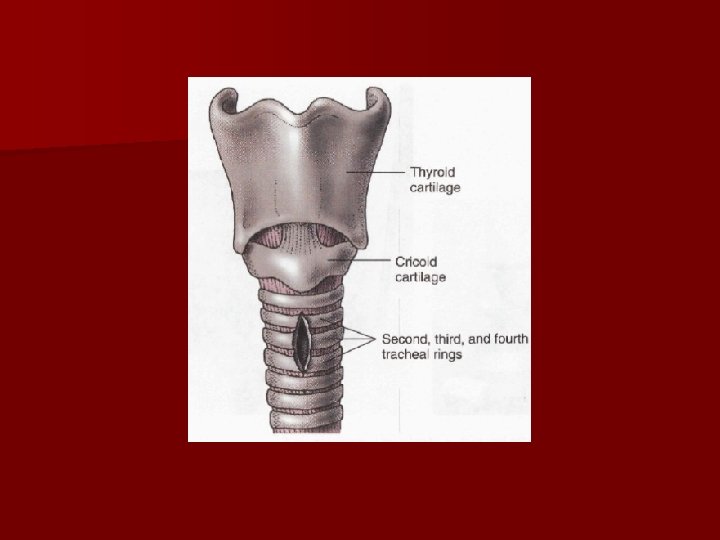
TRACHEOSTOMY Tracheotomy is the surgical incision into the trachea for the purpose of establishing an airway. n Tracheostomy is the (tracheal) stoma, or opening, that results from the tracheotomy. A tracheostomy can be performed as an emergency procedure or as a scheduled surgical procedure and can be temporary or permanent n Indications for tracheostomy
Complications n Tube obstruction n Tube dislodgment or accidental decannulation n Pneumothorax n Subcutaneous emphysema n Bleeding n Infection
Tracheostomy tubes n Double-lumen tube n Single-lumen tube n Cuffed tube n Cuffless tube n Fenestrated tube n Cuffed fenestrated tube n Metal tracheostomy tube n Talking tracheostomy tube
Dual-lumen cuffed tracheostomy tube with disposable inner cannula
Single-lumen cannula cuffed tracheostomy tube
Dual-lumen cannula cuffed fenestrated tracheostomy tube
Care Issues for the Tracheostomy Client n Prevention of tissue damage – Cuff pressure can cause mucosal ischemia. – Use minimal leak technique and occlusive technique. – Check cuff pressure often. – Prevent tube friction and movement. – Prevent and treat malnutrition, hemodynamic instability, or hypoxia.
Air Warming and Humidification n The tracheostomy tube bypasses the nose and mouth, which normally humidify, warm, and filter the air. n Air must be humidified. n Maintain proper temperature. n Ensure adequate hydration.
Suctioning n Suctioning maintains a patent airway and promotes gas exchange. n Assess need for suctioning from the client who cannot cough adequately. n Suctioning is done through the nose or the mouth. n Suctioning can cause: – – – Hypoxia (see causes to follow) Tissue (mucosal) trauma Infection Vagal stimulation and bronchospasm Cardiac dysrhythmias from hypoxia caused by suctioning
Causes of Hypoxia in the Tracheostomy n Ineffective oxygenation before, during, and after suctioning n Use of a catheter that is too large for the artificial airway n Prolonged suctioning time n Excessive suction pressure n Too frequent suctioning
Possible Complications of Suctioning n Tissue trauma n Infection of lungs by bacteria from the mouth n Vagal stimulation: stop suctioning immediately and oxygenate client manually with 100% oxygen n Bronchospasm: may require a bronchodilator
Tracheostomy Care n Assessment of the client n Secure tracheostomy tubes in place n Prevent accidental decannulation
Bronchial and Oral Hygiene n Turn and reposition every 1 to 2 hours, support out-of-bed activities, encourage early ambulation. n Coughing and deep breathing, chest percussion, vibration, and postural drainage promote pulmonary cure. n Oral hygiene—avoid glycerine swabs or mouthwash that contains alcohol; assess mouth for ulcers, bacterial or fungal growth, or infections.
Nutrition n Swallowing can be a major problem for the client with a tracheostomy tube in place. n If balloon is inflated, it can interfere with the passage of food through the esophagus. n Elevate head of bed for at least 30 minutes after client eats to prevent aspiration during swallowing.
Speech and Communication n Client can speak with a cuffless tube, fenestrated tube, or cuffed fenestrated tube that is capped or covered. n Client can write. n Phrase questions to client for “yes” or “no” answers. n A one-way valve that fits over the tube and replaces the need for finger occlusion can be used to assist with speech.
Weaning from a Tracheostomy Tube n Weaning is a gradual decrease in the tube size and ultimate removal of the tube. n Cuff is deflated as soon as the client can manage secretions and does not need assisted ventilation. n Change from a cuffed to an uncuffed tube. n Size of tube is decreased by capping; use a smaller fenestrated tube. n Tracheostomy button has a potential danger of getting dislodged.